17 Additional Information
This section provides supplemental information for Section 6 on media-specific occurrence, Section 7.1 for human health effects, and for Section 9 on site risk assessment.
17.1 Additional Information for Media-Specific Occurrence
This section includes links for the tables of media-specific occurrence information that are summarized in Section 6 and included in the figures in that section.
- Tables 17-1 A-C – outdoor air, indoor air, settled dust, precipitation
- Tables 17-2 A-C – soil, sediment, and biosolids
The Section 6 interactive plots webpage provides additional information for the data included in the figures. The interactive figures were developed using R software and plotly.
The previous version of Section 6 (June 2022) is archived as a PDF under Archived External Tables and Sections on the home page of this site. The previous version of Section 17.1 (June 2022) is archived as a PDF under Archived External Tables and Sections on the home page of this site.
Table numbers 17-3, 17-4, and 17-5 are reserved for future updates in media-specific occurrence.
17.2 Additional Information for Human Health Effects
This section supplements information provided in Section 7.1 on biomonitoring, exposure, toxicokinetic, toxicology, and epidemiology data for long-chain and short-chain PFAAs. The PFAS discussed in Sections 17.2.3 and 17.2.4 include perfluorocarboxylic acids (PFCAs) with four to fourteen carbons and perfluorosulfonic acids (PFSAs) with four or more carbons. Also covered are two per- or polyfluorinated ether carboxylates (FECAs)—ammonium 2,3,3,3-tetrafluoro-2-(heptafluoropropoxy)propanoate (also known as perfluoro-2-propoxypropanoic acid (PFPrOPrA); hexafluoropropylene oxide [HFPO] dimer acid, commonly known as GenX) (Section 2.2.3.5); and 4,8-dioxa-3H-perfluorononanoate (commonly known as ADONA); and per- and polyfluoroether carboxylates (PFECAs); per- and polyfluoropolyether carboxylates (PFPECAs) including chlorinated PFPECAs (ClPFPECAs); per- and polyfluoroether sulfonates (PFESAs) including chlorinated PFESAs; per- and polyfluoropolyether sulfonates (PFPESAs), fluorotelomer alcohols, and fluorotelomer sulfonic acids. These PFAS that contain ether group(s) are replacements for PFOA, PFNA, and/or PFOS as processing aids in certain fluoropolymer production, and some are also formed as industrial byproducts. They are included because they are of current interest and health effects data are available. There is little or no publicly available health effects information for most of the many other PFAS used in commerce (Section 2.5), including precursors that can be converted to PFAAs in the environment and in the human body.
For further detail of scientific names and carbon chain length of PFAAs see Section 2.2.
17.2.1 Overview
Based on the number of studies located through searches of the National Library of Medicine’s PubMed, a database containing relevant peer-reviewed publications, much of the information summarized here became available after 2005. Additional studies may be available, particularly for those compounds with large health effects data sets, and additional information on the topics in this section can be found in databases such as PubMed and references listed in Section 7.1.
The publicly available toxicological data set is currently largest for PFOA and PFOS, with considerable data also available for PFBA, PFBS, PFHxA, PFNA, PFDA, and GenX. Fewer studies are available for PFHxS, PFUnA, PFDoA, ADONA, and the other ether and polyether PFAS mentioned above, and little or no data for PFPeA, PFHpA, PFTrA, PFTA, PFPeS, PFHpS, PFNS, or PFDS. Most of the mammalian studies were conducted in rodents, with a few in nonhuman primates (monkeys). The most notable toxicological effects from the mammalian studies of these PFAS, with relevant citations, are discussed in Section 17.2.5 and are summarized in Table 17-8 Toxicological Effects Excel file (last updated November 2021). However, due to the large size of the toxicological data set, it is beyond the scope of this section to identify no observed adverse effect levels (NOAELs) and lowest observed adverse effect levels (LOAELs) for these effects. The numerous reviews of potential epidemiological associations of health endpoints with PFAAs are discussed in Section 17.2.4. Many of the epidemiology studies evaluate associations of health endpoints with multiple PFAAs detected in the blood serum of the subjects. Epidemiologic data from the general population have been used to develop draft reference doses for PFOA and PFOS (CA OEHHA 2023; USEPA 2023), as well as for PFHxS and PFDA (USEPA 2023), and draft cancer slope factors for PFOA (USEPA 2023; CA OEHHA 2023) based on human data.
Finally, data gaps and research needs are discussed.
17.2.2 Human Biomonitoring and Sources of Exposure
Several long-chain PFAAs (from highest to lowest geometric mean [GM] serum levels, as follows: PFOS, PFOA, PFHxS, PFNA) are present in the low parts per billion (ng/ml) range in the blood serum of almost all adult residents of the United States, while other PFAS are detected in a smaller percentage of the population (CDC 2022; Olsen et al. 2017)). In contrast, short-chain PFAAs such as PFBS and PFHxA are more rapidly excreted and were infrequently detected in the blood serum of the U.S. general population (CDC 2022; Olsen et al. 2017). For example, PFBS was detected in less than 5% of serum samples in all National Health and Nutrition Examination Survey (NHANES) years except 2005–‘06 (CDC 2022). Both NHANES and the blood donor studies show generally higher levels of long-chain PFAAs in males than females, with generally decreasing serum levels of long-chain PFAAs over time. NHANES 2013–‘14 evaluated PFAS in children 3–11 years old (CDC 2022) and found serum levels of PFOS, PFOA, PFHxS, and PFNA generally similar to those in older adolescents and adults in the same time period. It was noted that most of the children studied were born after PFOS manufacturing was phased out in the United States in 2002 (Ye et al. 2018). Long-chain PFAA human serum levels in other industrialized countries are generally similar to the United States (Kato 2015) and may be lower in less developed nations (for example, Afghanistan) where they are less likely to be used industrially and consumer products containing them are less frequently used (Hemat et al. 2010). Testing in 2017 by the North Carolina Department of Health and Human Services (NC DHHS) did not detect HFPO-DA (“GenX”) in the blood serum or urine of North Carolina residents with previous or current exposure from private wells, but did detect other PFAS (NC DHHS 2018). A North Carolina State University study of a public water system and its users included a larger list of PFAS analytes and, although no GenX was detected, they identified four newly identified PFAS in the drinking water and blood serum of most participants (Hogue 2019; Hopkins et al. 2018). A study of a potentially exposed population detected ADONA in only a few subjects (Fromme et al. 2017).
Human exposures can result from consumption of fish from waters contaminated with bioaccumulative PFAAs (for example, MDCH 2014). PFSAs with more than eight fluorinated carbons (that is, PFOS and longer chain for PFSAs; PFNA and longer chain for PFCAs) are substantially more bioaccumulative than shorter chain PFAAs, with PFSAs generally more bioaccumulative than PFCAs with the same number of fluorinated carbons (Conder et al. 2008; Martin et al. 2003). When drinking water is contaminated with even relatively low levels of long-chain PFAAs, exposure from drinking water may dominate contributions from exposure sources such as food and consumer products that are prevalent in the general population. For example, USEPA (2011) predicted that ongoing exposure to 20 ng/L PFOA in drinking water will increase serum PFOA levels more than two-fold from the U.S. median of 2 ng/L. Elevated serum levels of long-chain PFAAs have been observed in communities with contaminated drinking water in several U.S. states, including Ohio and West Virginia (WV University 2008; Emmett et al. 2006; Steenland et al. 2009) (Hoffman et al. 2011), New Hampshire (NH DHHS 2015), Alabama (ATSDR 2013), Minnesota (MDH 2009; Landsteiner et al. 2014), New York (NYS DOH 2016), and in other nations, including Germany (Hölzer et al. 2008) and Sweden (Li et al. 2018) (Table 17-6). ATSDR (2022) has conducted exposure assessments that included biomonitoring in eight U.S. locations impacted by PFAS in drinking water.
Understanding exposures to PFAS at different developmental phases (for example, fetus, infant) is important to ensure protection of the most sensitive subpopulations. Evidence for developmental effects from early life exposures to long-chain PFAAs in humans is discussed in Section 17.2.4 and in animals in Section 17.2.5. PFAAs (primarily PFHpA and longer chain PFCAs; PFHxS and longer chain PFSAs) have been detected in human amniotic fluid (Stein et al. 2012; Zhang et al. 2013), umbilical cord blood (Kato 2015; Kudo 2015), and breast milk (Liu et al. 2010; White et al. 2011; Post, Cohn, and Cooper 2012; Kato 2015; Kudo 2015). Although the specific compounds analyzed for and/or detected vary among studies, other PFAAs that have been analyzed for in breast milk rarely exceeded the limit of quantitation (Tao et al. 2008; Tao et al. 2008). Serum levels of several long-chain PFAAs were higher in breast-fed infants than in their mothers and declined slowly following weaning (Fromme et al. 2010), and serum levels of infants who drank formula prepared with PFAS-contaminated water are predicted to be higher than in older individuals using the same water source (Goeden, Greene, and Jacobus 2019). Infants and toddlers may also receive higher exposures because of age-specific behaviors such as hand-to-mouth activity that results in greater ingestion of house dust, and more time spent on floors with treated carpets relative to older children or adults (Trudel et al. 2008; Shoeib et al. 2011).
Elevated serum levels of PFAAs, in some cases >100,000 ng/ml, have been found in industrially exposed workers (Olsen 2015). Serum concentrations of PFCAs (PFHpA and longer) were also increased in professional ski waxing technicians due to exposures to fluorinated ski waxes (Freberg et al. 2010; Nilsson et al. 2010). Higher serum levels of PFDA (Dobraca et al. 2015), PFOS, and PFHxS (Rotander et al. 2015) have been reported in firefighters relative to those in the general population.
17.2.3 Toxicokinetics
PFAAs for which data are available (PFOA, PFHpA, PFHxA, PFOS) were well absorbed orally (>90%) in rodents (Kudo 2015). PFOA and PFNA were absorbed via inhalation as dusts or aerosols (Kinney, Chromey, and Kennedy 1989; Hinderliter, DeLorme, and Kennedy 2006). PFOA was absorbed to a limited extent from dermal exposure in studies of isolated human and rodent skin (Fasano et al. 2005; Franko et al. 2012). Several recent in vivo studies demonstrate dermal absorption in laboratory animals and humans. Chen et al. (2022) reported that the tested PFAS (PFCAs with 4 to 12 carbons; PFBS, PFHxS, PFOS; 6:2- and 8:2 diPAP) were absorbed after a single application to skin; the extent of dermal absorption varied with compound and dose. Weatherly et al. (2023) reported toxicity and gene expression changes in liver and skin, as well as detection in urine and serum, after daily application of PFPeA, PFHxA, and PFHpA to the skin of mice for 28 days. Abraham and Monien (2022) demonstrated dermal absorption of isotopically labelled PFOA mixed with sunscreen in a human volunteer. Section 1.4.3 includes information about dermal uptake of PFAS in the environment. Section 1.4.2.3 includes information about potential PFAS exposures from cosmetics and personal care products including sunscreen.
PFAAs, particularly long-chain PFCAs and PFSAs, have unique toxicokinetic properties as compared to other types of POPs. Unlike most other bioaccumulative organic compounds (for example, dioxins, PCBs), PFAAs do not have a high affinity for adipose tissue. In contrast, PFAAs are water soluble, have an affinity for proteins (which varies among compounds), and generally distribute primarily to the liver, blood serum (where they are bound to albumin and other proteins), and kidney (Bischel et al. 2011; Lau 2012, 2015; Kato 2015).
PFAAs are highly resistant to chemical reactions. As such, they are not metabolized, and this is also true for HFPO-DA (Gannon et al. 2016) and ADONA (Gordon 2011). However, PFAA precursors can be metabolized to PFAAs within the body, and reactive intermediates may be formed in these metabolic pathways (Rand and Mabury 2016). Some examples are the metabolism of 6:2 fluorotelomer alcohol (6:2 FTOH) to PFBA, PFPeA, PFHxA, and PFHpA (Buck 2015); 8:2 FTOH to PFOA and PFNA (Kudo 2015; Kabadi et al. 2018); and perfluorooctane sulfonamidoethanols (FOSEs), perfluorooctane sulfonamides (FOSAs), and perfluorooctane sulfonamidoacetic acids (FOSAAs) to PFOS (Gebbink, Berger, and Cousins 2015). Additionally, larger PFAS molecules such as polyfluoroalkyl phosphoric acid diesters (diPAPs) have been found in human blood serum and can be metabolized to FTOHs, which are further metabolized to PFCAs (D’Eon and Mabury 2011; Lee and Mabury 2011).
Table 17-6. Long-chain PFAA serum levels in populations exposed through drinking water (ng/ml = µg/L = ppb)
(Means, medians, and maximums available from the cited studies are shown. AM–arithmetic mean; GM–geometric mean; 95th–95th percentile; — indicates that data are not available)
| Location | Study Population | Attributed Source | Year | PFOA | PFOS | PFHxS | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Median | Max. | Mean | Median | Max. | Mean | Median | Max. | ||||
| C8 Study Population: WV/Ohio (WV University 2008) Includes occupationally exposed subject |
n = ~69,000 <1 – >90 yrs. M-48%, F-52% |
Industrial–PFOA | 2005–06 | 83 (AM) | 28 | 22,412 | 23 (AM) | 20 | 759 | — | — | — |
| Arnsberg, Germany (Hölzer et al. 2008) |
n=90 Children 5–6 yrs. |
Industrial waste applied to agricultural land–mainly PFOA |
2006 | 25 (AM) | — | 97 | 5 (AM) |
— | 21 | 1 (AM) |
— | 13 |
|
n=164 Mothers 23–49 yrs. |
27 (AM) | — | 100 | 6 (AM) |
— | 17 | 1 (AM) |
— | 6 | |||
|
n=101 Men 18–69 yrs. |
29 (AM) | — | 78 | 12 (AM) |
— | 36 | 3 (AM) |
— | 9 | |||
| East Metro, MN (MDH 2009) |
n = 196 20–86 yrs. M-45%, F-55% |
Industrial–multiple PFAS |
2008–09 | 23 (AM) | 16 | 177 | 48 (AM) | 41 | 448 | 15 (AM) |
9 | 316 |
| Decatur, AL (ATSDR 2013) |
n=153 “child” – >60 yrs. M-41%, F-59% |
Industrial–multiple PFAS |
2010 | 16 (GM) | — | 144 | 40 (GM) |
— | 472 | 6 (GM) |
— | 59 |
| Ronneby, Sweden (Li et al. 2018) |
n = 3418 4–83 yrs. M-47%, F-53% |
AFFF | 2014 | 14 (AM) | 10 | 92 | 245 (AM) | 176 | 1,870 | 228 (AM) | 152 | 1790 |
| Portsmouth, NH (NH DHHS 2015) |
n = 108 < 12 yrs. |
AFFF | 2015 | 4 (GM) |
5 | 12 | 9 (GM) |
9 | 31 | 6 (GM) |
7 | 26 |
|
n= 363 >12 yrs. |
3 (GM) |
— | 16 | 8 (GM) |
— | 75 | 8 (GM) |
— | 75 | |||
| Hoosick Falls, NY (NYS DOH 2016) |
n = 2,081 <17 – >60 yrs. M-45%, F-55% |
Industrial–PFOA | Feb.–April 2016 | 24 (GM) |
28 | — | — | — | — | — | — | — |
| Merrimack, NH (NH DHHS 2017) |
Public water system n = 217 |
Industrial–PFOA | 2016 | 3.9 (AM) |
— | 10.1 (95th) |
5.5 (AM) |
— | 15.2 (95th) |
1.3 (AM) |
— | 3.2 (95th) |
|
Private wells N=219 |
4.4 (AM) |
— | 26.6 (95th) |
5.4 (AM) |
— | 16.4 (95th) |
1.3 (AM) |
— | 3.4 (95th) |
|||
Excretion of PFAAs and HFPO-DA is primarily through the urine, with a much smaller percentage, if any, eliminated in the feces. In women of childbearing age, excretion also occurs through menstruation and lactation (Harada and Koizumi 2009; Thomsen et al. 2010). Serum PFAS levels were lower in adult males undergoing venesection (ongoing blood withdrawal) for medical reasons (Lorber et al. 2015) and in firefighters who had donated blood, as compared to other firefighters (Rotander et al. 2015). The excretion rate for long-chain PFAAs varies substantially between animal species, and it is much slower in humans than in laboratory animals. Additionally, for some PFAS, including PFOA, PFNA, and others, the excretion rate is very different in males and females of the same rodent species, likely due to differences in the extent of secretion and reabsorption by organic anion transporter proteins (OATs) and possibly other transporter proteins in the kidney, reviewed in Lau (2012); Lau (2015); Kudo (2015); and USEPA (2023). Half-lives in rodents, nonhuman primates, and humans for the PFAS included in this section are shown in Table 17-7.
Table 17-7. Half-lives of PFCAs, PFSAs, and perfluoroethers in rodents, nonhuman primates, and humans
Notes: No information was located for PFPeA, PFDoA, PFTrDA, PFTeDA, PFPeS, PFNS, PFDS, ADONA; — indicates that data are not available; h–hour, d–day, y–year.
| Mouse | Rat | Nonhuman primate | Human | |||||
|---|---|---|---|---|---|---|---|---|
| Male | Female | Male | Female | Male | Female | Male | Female | |
| PFCAs | ||||||||
| PFBA | 13 ha | 2.9 ha | 9.2 ha | 1.8 ha | 40 ha | 41 ha | 72 ha (O; mean) | 87 ha (O; mean) |
| PFHxA | ~1 hb | ~2 hc | ~2 hc | 5.3 hc | 2.4 hc | 32 de (O; GM) | — | |
| 14–47 hd | ||||||||
| PFHpA | —- | —- | 2.4 hf | 1.2 hf | —- | —- | — | <50 yrs. of age-1.2 yg (G-U) |
| All M & F >50 yrs. of age-1.5 yg (G-U) | ||||||||
| PFOA | 19 dh | 17 dh | 4–6 di | 2-4 hi | 21 dj | 30 dj |
3.8 y (O; mean); 2.4 y (O; GM)k |
|
| 15–50 yrs. of age-4.6 yn (DW) | 15–50 yrs. of age-3.1 yn (DW) | |||||||
| PFNA | 34–68 do,p | 26–69 do,p |
30 do,p
|
1–2 do,p | —- | —- | <50 yrs. of age-2.5 yg (G-U) | |
| All M & F >50 yrs. of age-4.3 yg (G-U) | ||||||||
| PFDA | —- | —- | 24 dq | 29 dq | —- | —- | <50 yrs. of age-4.5 yg (G-U) | |
| All M & F >50 yrs. of age-12 yg (G-U) | ||||||||
| PFUnA | —- | —- | —- | —- | —- | —- | <50 yrs. of age-4.5 yg (G-U) | |
| All M & F >50 yrs. of age-12 yg (G-U) | ||||||||
| PFSAs | ||||||||
| PFBS | —- | —- | 3.1–4.5 hr,s | 2.4–4.0 hr,s | 15–95 hr,s | 8.1–83 hr,s | 26 d (O; GM)s | |
| PFPeS | —- | —- | —- | —- | —- | —- | 1.03 yz(DW; median) | |
| PFHxS | 29 dt | 26 dt | 29 dt | 1.8 hdt | 141 dt | 87 dt |
8.5 y (O; mean); 7.3 y (O, GM)k |
|
| 15–50 yrs. of age-7.4 yn (DW) | 15–50 yrs. of age-4.7 yn (DW) | |||||||
| PFHpS | —- | —- | —- | —- | —- | —- | 5.0 yz(DW; median) | |
| PFOS | 40 du | 34 du | 47–67 du,v | 40–48 du,v | 132 du | 110 du |
5.4 y (O; mean); 4.8 y (O; GM)k |
|
| 15–50 yrs. of age-4.6 yn (DW; mean) | 15–50 yrs. of age-3.1 yn (DW; mean) | |||||||
| Perfluoroether (Replacement for PFOA in fluoropolymer manufacturing processes) | ||||||||
| GenX | 21 hw | 18 hw | 3 hx | <3 hx | ~2 hy | ~2 hy | —- | —- |
| PFOS-branched isomers | —- | —- | —- | —- | —- | —- | 2.87–5.57 yz(DW, GM) | |
| DW–Based on decline in serum levels after exposure to contaminated drinking water ended. GM–Geometric mean. G-U–Mean value; based on urinary excretion in general population, with modeled menstrual excretion for F < 50 yrs. old. More uncertain than estimates based on decline in serum levels. (Not shown for PFAS with half-lives based on serum decline). O–based on decline in serum levels in workers or retired workers after exposure ended. a Chang et al. (2008) b Iwai (2011), reported in Russell, Nilsson, and Buck (2013) c Chengelis et al. (2009) d Noker (2001), reported in Russell, Nilsson, and Buck (2013) e Russell, Nilsson, and Buck (2013) f Ohmori et al. (2003) g Zhang et al. (2013) h Johnson and Ober (1979); Kemper and Jepson (2003) i Lau et al. (2006) j Butenhoff et al. (2004) k Olsen et al. (2007) l Bartell et al. (2010) m Brede et al. (2010) n Li et al. (2018) o Tatum-Gibbs et al. (2011) p Ohmori et al. (2003) q Gibbs et al. (2012) r Chengelis et al. (2009) s Olsen et al. (2009) t Sundstrom et al. (2012) u Chang et al. (2012) v Butenhoff (2007) w DuPont (2011) x DuPont (2011) y DuPont (2008) |
||||||||
As shown in Table 17-7, excretion rates in mammalian species vary among PFAS for which half-life data are available, with short-chain PFAAs and GenX generally excreted more rapidly than longer chain PFAAs. Half-lives in rodents and nonhuman primates are generally in the range of several weeks to several months for long-chain PFAAs, and about 1 hour to several days for short-chain PFAAs and GenX. However, PFOA, PFNA, and PFHxS (reviewed in Kudo 2015) are excreted much more rapidly (hours to days) in female than male rats; this sex difference in rats also exists but is not as pronounced for PFBA, PFHxA, PFHpA, and PFBS (Kudo 2015). This difference in excretion rate is important in interpretation of rat toxicology studies of these compounds, particularly for developmental effects.
Human half-lives for PFAS are longer than in other mammalian species that have been studied, with estimates of several years for long-chain PFAAs (PFOA, PFNA, PFOS, PFHxS); 1 year for PFHpA, and several days to 1 month for shorter chain PFAAs (PFBA, PFHxA, PFBS; Table 17-7). The estimates of human half-life shown in Table 17-7 are based on measured declines in serum PFAS levels in the same individuals over time after a source of elevated exposure, such as occupational exposure or ingestion of contaminated drinking water, ceases. Such estimates are less uncertain than population-based estimates from modeling of PFAS intake and biomonitoring data for serum PFAS levels from different sets of individuals from the general population at different time points. Half-life estimates based on urinary excretion are available for several PFAAs, including some with no serum-based half-life estimates ((Zhang et al. 2013) shown as G-U in Table 17-7); these urinary estimates are less certain because they include modeled estimates of menstrual excretion in women of childbearing age and do not consider fecal excretion or blood loss other than menstruation (for example, blood donation). It should be noted that there are large inter-individual variations in human half-lives, which may arise from physiological factors (for example, differences in renal transport by OATs; Yang, Glover, and Han 2010).
Because of the large species and sex differences in excretion rates, the internal dose resulting from a given administered dose varies widely among species and, in some cases, males and females of the same species. Therefore, interspecies (for example, animal-to-human) comparisons must account for the large interspecies half-life differences with approaches such as use of internal dose (as indicated by serum level) as the dose metric, interspecies toxicokinetic extrapolation based on the ratio of half-lives in humans and animals, or use of physiologically based pharmacokinetic models.
17.2.3.1 Toxicokinetics Relevant to Developmental Exposures
Toxicokinetics relevant to developmental exposures to PFAAs are important because developmental effects are sensitive endpoints for toxicity of long-chain PFAAs in rodents, and prenatal exposure to some long-chain PFAA was associated with decreased fetal growth in some human epidemiology studies (see Section 17.2.3.4). Developmental exposures have been studied in rodents for several PFAAs, but not in nonhuman primates. PFAAs cross the placenta to reach the developing fetus in both humans and rodents (reviewed in Lau 2012 and Kudo 2015), and are transferred to milk, resulting in exposure via lactation (Luebker et al. 2005; White et al. 2009; Kato 2015). In humans, long-chain PFAAs have been detected in cord blood (for example, Wang et al. 2019) and amniotic fluid (Stein et al. 2012; Zhang et al. 2013).
In humans, the greatest exposures to PFAAs in breast milk occur during the first few months of infancy because both PFAA concentrations in milk and the breast milk ingestion rate on a BW basis (ml/kg/day) are highest then; PFAA levels in milk may be lower in mothers who previously nursed other infants (Tao et al. 2008; Haug et al. 2011; Thomsen et al. 2010). Serum concentrations of long-chain PFAAs in breast-fed infants increase several-fold from the levels at birth during the first few months of life, followed by a decline in older infancy and early childhood (Fromme et al. 2010; Mogensen et al. 2015; Verner et al. 2016, 2016; MDH 2018, 2019; reviewed in NJDWQI 2015, 2017, 2018). Because of their higher rate of fluid consumption on a BW basis (USEPA 2019), exposures to infants who consume formula prepared with PFAS-contaminated water are also highest during the first few months of life. Goeden, Greene, and Jacobus (2019) presented a model that predicts transplacental transfer and exposure to breast-fed and formula-fed infants for long-chain PFAAs in drinking water.
17.2.3.2 Relationship of Human Exposures to Serum Levels
Clearance factors (CL) that describe the relationship between oral exposures or dose (ng/kg/day) and steady-state serum levels (ng/L) in humans have been developed for PFOA (Lorber and Egeghy 2011; USEPA 2016) and PFOS (USEPA 2016):
Dose [ng/kg/day] x CL [L/kg/day] = serum concentration [ng/L].
These clearance factors, which indicate bioaccumulative potential, are based on average values for human PFAS half-lives and volumes of distribution (Vd);
CL [L/kg/day] = Vd [L/kg Body Wt] x [Ln2/half-life in days].
Where Ln2 is the natural log of 2.
When combined with mean daily U.S. water ingestion rates (USEPA 2011), the CLs have been used to predict the expected average increase in serum levels (above the “baseline” serum level from non-drinking water sources) that results from ongoing exposure to a given drinking water concentration of PFOA or PFOS (Bartell 2017; NJDWQI 2017; Post, Gleason, and Cooper 2017). For PFOA, this average serum:drinking water ratio was predicted to be greater than 100:1 (NJDWQI 2017); this ratio is consistent with data from exposed populations and toxicokinetic modeling (Emmett et al. 2006; Hoffman et al. 2011; Bartell 2017). The CL for PFOS predicts an average serum:drinking water ratio of about 200:1 (NJDWQI 2018; Post, Gleason, and Cooper 2017; Lu and Bartell 2020), and available toxicokinetic data also support an estimated ratio of 200:1 for PFNA (NJDWQI 2015; Lu and Bartell 2020) and PFHxS (Lu and Bartell 2020). It should be noted that PFAA serum:drinking water ratios vary among individuals using the same source of contaminated drinking water, due to inter-individual differences in daily water consumption rates (L/kg/day) and/or physiological differences relevant to toxicokinetics.
Bartell (2017), Lu and Bartell (2020), and ATSDR (2022) have developed online calculators that provide estimates of an individual’s serum concentrations of PFOA, PFOS, PFNA, and PFHxS from the information that is entered, including drinking water levels of these PFAS and other relevant factors. These estimates are based on long-term exposure to a constant drinking water concentration and that serum PFAS concentrations are impacted by interindividual variability in both toxicokinetic factors (for example, PFAS half-lives) and daily drinking water ingestion rate.
17.2.3.3 Isomer-Specific Toxicokinetics
Some PFAAs exist as a mixture of linear and branched isomers; the isomer profile varies depending on the manufacturing process used (telomerization yields primarily linear PFAS; electrochemical fluorination yields a mixture of linear and branched PFAS; Section 2.2.5.2. Toxicokinetics may differ among isomers of the same PFAA in rodents (Loveless et al. 2006; De Silva et al. 2009) and humans (Zhang et al. 2013; Gao et al. 2015; Beesoon et al. 2011; Xu et al. 2020; Li et al. 2022).
17.2.4 Human Epidemiology Studies
As discussed in Section 7.1.3, the epidemiological database for long-chain PFAAs, particularly PFOA and PFOS, is more extensive than for many other environmental contaminants. Many of the studies are recent, and the number of available studies is constantly increasing. In contrast, there are few or no epidemiology studies for many other PFAS (Carlson et al. 2022; Radke et al. 2022).
Many U.S. general population studies are based on data from NHANES (CDC 2022), and other general population studies come from various worldwide locations. These include studies of specific subpopulations such as pregnant women, infants, children, or the elderly, as well as evaluations of associations of prenatal exposures with effects later in life. Data on communities exposed to PFOA through contaminated drinking water come primarily from the C8 Health Study evaluations of approximately 70,000 Ohio and West Virginia residents exposed in drinking water for at least 1 year at concentrations of 50 ng/L to >3,000 ng/L, including evaluations by the C8 Science Panel (Frisbee et al. 2009; C8 Science Panel 2020). This panel consisted of three prominent environmental epidemiologists charged with determining whether there are “probable links” (defined as “given the scientific evidence available, it is more likely than not that a connection exists between C8 exposure and a particular human disease among class members”) between PFOA exposures in this study group and disease. Researchers who participated in the C8 Science Panel recently evaluated current epidemiologic evidence for PFOA and the diseases for which the C8 Science Panel had concluded in 2011–12 that there was a “probable link” with PFOA exposure (kidney and testicular cancer, high cholesterol, thyroid disease, pregnancy-induced hypertension, ulcerative colitis; C8 Science Panel Probable Link reports (C8 Science Panel 2017). They also reviewed evidence for associations of PFOA and additional health effects (Steenland et al. 2020). The conclusions of Steenland et al. (2020) for specific health effects are discussed below.
Until recently, health effects studies were not available from communities with drinking water contaminated with either the other PFAS discussed in this section or the complex mixtures of PFAS present in AFFF. Studies of associations of PFAS with a variety of health effects in a community exposed to AFFF-contaminated drinking water in Sweden have now been reported (Andersson et al. 2019; Li et al. 2020, 2021, 2022; Xu et al. 2020, 2022; Hammarstrand et al. 2021; Nielsen and Joud 2021; Engstrom et al. 2022; Nielsen et al. 2022). Additional epidemiological studies of seven communities exposed to PFAS found in AFFF or specific PFAS other than PFOA (for example, PFNA) are now being conducted through the ATSDR-funded multisite study (ATSDR 2022). Section 1.4.1 includes information about potential human health effects from PFAS exposure arising from AFFF in drinking water.
Finally, health effects of several long-chain PFAAs, including PFOA, PFOS, and PFNA, have been studied in occupationally exposed workers (Khalil 2015). Because these workers were primarily male, relatively few women were included in these studies.
Exposure assessment in most but not all of the epidemiology studies of PFAS is based on blood serum levels of PFAS as an indicator of internal dose. The studies often evaluate associations between health endpoints and multiple PFAS detected in blood. Serum levels of long-chain PFAAs are indicators of long-term exposures (Section 7.1.2) that reflect individual differences in both exposure (for example, daily water consumption) and rate of excretion. Therefore, serum levels are less uncertain as indicators of exposure than external parameters such as drinking water concentration. In contrast to long-chain PFAS, there is little epidemiological information on short-chain PFAS because they are infrequently detected in blood serum due to their more rapid excretion. Exposure assessment in some of the C8 studies of communities with PFOA exposure from an industrial source is based on serum PFOA levels estimated from modeling of drinking water and air PFOA concentrations over time, rather than measured serum levels Savitz et al. 2012; Winquist and Steenland 2014, 2014; Dhingra et al. 2016, 2016; Herrick et al. 2017). Finally, exposure is based on job classification, rather than serum PFAA measurements in some occupational studies of PFOA (Gilliland and Mandel 1993; Leonard 2003; Lundin et al. 2009; Raleigh et al. 2014), PFNA (Mundt et al. 2007), and PFOS (Alexander et al. 2003; Olsen et al. 2004; Alexander and Olsen 2007; Grice et al. 2007).
As is the case for epidemiologic studies of environmental contaminants in general, the human studies of PFAAs are observational, in contrast to toxicology studies, which are experimental. Additionally, most epidemiology studies of PFAAs are cross-sectional, although some use other designs (prospective, retrospective, case-control). In cross-sectional studies, exposure and outcome are evaluated at the same point in time. Such cross-sectional studies cannot reveal whether increased exposure led to the health endpoint or vice versa, and reverse causality (for example, when a physiological change affects serum PFAS levels, rather than the serum PFAS levels causing the physiological change) has been hypothesized by some researchers as partially or totally explaining some of the associations in the epidemiological literature, including reduced birth weight and decreased kidney function (reviewed in NJDWQI 2017). In general, publications of epidemiology studies report results in terms of associations with the endpoints of interest based on statistical analysis. When there are multiple studies of associations of an environmental contaminant such as PFAA(s) with a health endpoint, results often differ among studies. The differing results can arise from difference in the study design (for example, sex, age, ethnicity of population studied; magnitude and/or duration of exposure; method for assessment of endpoint of interest), size of population studied (may be too small to detect statistically significant associations), method used for statistical analysis, consideration of potential confounding factors, or chance.
Therefore, conclusions about whether the overall body of evidence supports an association are based on scientific judgment and may differ among scientists who review the same body of data. Additionally, for PFAS, because many new epidemiology studies continually become available, more recent evaluations may include considerable data not available for earlier evaluations. Because observational studies are not designed to prove causality for health effects, conclusions about evidence for causality are based on criteria, such as the Hill criteria (Lucas and McMichael 2005) related to the overall body of relevant scientific information (for example, consistency, dose-response, biological plausibility, potential for reverse causality). For example, observations of associations with the same health endpoint in studies from multiple locations and in different types of populations (for example, general population, exposed communities, workers), as is the case for some effects associated with PFOA and PFOS (Post, Cohn, and Cooper 2012; USEPA 2023; USEPA 2023) strengthen the weight of evidence for that effect. Use of systematic review methods are increasingly used to evaluate the quality of epidemiological studies as well as the potential confounders (for example, USEPA 2023). As is the case for associations, conclusions about causality may differ among scientists reviewing the same body of data.
17.2.4.1 Noncancer Health Endpoints
This section summarizes information for various categories of noncancer health endpoints: Changes in systemic markers, Fetal growth, Immune system effects, Thyroid effects, and Other effects.
Systemic Markers
For PFOA and PFOS (Khalil 2015; USEPA 2023, 2016; NJDWQI 2017, 2018; ATSDR 2021), PFNA (NJDWQI 2015; ATSDR 2021), and PFDeA (ATSDR 2021), the cited reviews concluded that associations are generally consistent for increases in total cholesterol and/or low-density lipoproteins. Australia Government DOH (2018) concluded, based on a review of key reports and published systematic reviews, that an association of both PFOA and PFOS with small changes in cholesterol is generally observed. Additionally, the C8 Science Panel concluded that there is a “probable link” between PFOA and clinically defined high cholesterol (C8 Science Panel 2012). Rappazzo, Coffman, and Hines (2017) concluded that the evidence for an association of prenatal or childhood exposure to PFAS with increased cholesterol is generally consistent; studies reviewed found associations with PFOA, PFOS, PFNA, and/or total PFAS. Regarding causality, NJDWQI (2017) concluded that the evidence supports multiple criteria for a causal relationship between increased serum cholesterol and PFOA, while Australia Government DOH (2018) concluded that it cannot be established whether PFOA or PFOS causes increased cholesterol based on currently available data. NASEM (2022) concluded that there is sufficient evidence for an association of PFAS with dyslipidemia in adults and children.
Steenland et al. (2020) noted continued consistent findings of an association between PFOA and high cholesterol. However, although high cholesterol is a risk factor for cardiovascular disease, the C8 Science Panel did not find a “probable link” for PFOA and heart disease, and subsequent studies have also not found an association. Relevant to this issue, Steenland et al. (2020) stated that this apparent inconsistency might be explained by associations of PFOA not only with increased cholesterol, but with increased high density lipoprotein (HDL) and decreased C-reactive protein, both of which decrease heart disease risk
Most reviews have concluded that PFOA (Gleason et al. 2015; Khalil 2015; 2023; NJDWQI; ATSDR 2021) and PFNA (NJDWQI 2015) are generally associated with increases in certain liver enzymes, particularly alanine aminotransferase (ALT). NJDWQI (2017) concluded that there is some evidence to support a causal relationship between PFOA and ALT. In contrast, most earlier evaluations of PFOS have found weaker or no evidence for associations with increased liver enzymes (Gleason et al. 2015; Khalil 2015; NJDWQI 2018, 2018. However, ATSDR (2021), p. 26, concluded that “increases in serum enzymes and decreases in serum bilirubin, observed in studies of PFOA, PFOS, and PFHxS, are suggestive of liver alterations.” NASEM (2022) concluded that there is limited or suggestive evidence for an association of PFAS with liver enzyme alterations in adults and children. For PFOA, USEPA (2023) concluded that there is consistent evidence of a positive association with ALT in adults, at median PFOA levels as low as 1.3 ng/mL. USEPA (2023), p. 3-28 to 3-29, concluded that “there is generally consistent evidence of a positive association between exposure to PFOS and ALT. However, one source of uncertainty in epidemiology studies of PFAS is confounding across the PFAS, as individuals are exposed to a mixture of PFAS and it is difficult to disentangle the effects. This cannot be ruled out in this body of evidence given the attenuation of the association in Lin et al. (2010), the only general population study that performed multi-pollutant modeling. … Thus, while there is evidence of an association between PFOS and ALT, there is residual uncertainty. ”Australia Government DOH (2018) concluded that an association of PFOA and PFOS with elevated levels of the liver enzyme ALT was observed in many studies. Steenland et al. (2020) also concluded that the limited currently available data do not support an association of PFOA and liver disease. However, Steenland et al. (2020) noted that the lack of human studies with sufficient power to detect this effect, well established liver toxicity of PFOA in experimental animals, bioaccumulation of PFOA in human liver, and extensive evidence for associations with markers of liver damage indicate the need for additional research, particularly in regard to potential associations with nonalcoholic fatty liver disease.
Various reviews have concluded that there is some evidence or limited evidence for an association of increased serum uric acid and/or hyperuricemia with exposure to PFOA, PFOS, and/or PFNA (Gleason et al. 2015; Khalil 2015; NJDWQI 2015, 2017, 2018; Australia Government DOH 2018).
Fetal Growth
Exposure to PFOA and PFOS were associated with relatively small changes in measures of decreased fetal growth (for example, birth weight, head circumference) in most studies, while some studies did not find such an association. A systematic review and meta-analysis by Johnson et al. (2014) found that there is “sufficient” human evidence that developmental exposure to PFOA reduces fetal growth in humans and provided a quantitative estimate of the decrease in birth weight per ng/ml serum PFOA. The main analysis included nine studies in which maternal or umbilical cord serum PFOA levels were measured in pregnant women. These studies met other inclusion criteria defined by the researchers; study subjects were from the general population in various locations. An additional analysis included a large study from the C8 Health Study population with exposure from contaminated drinking water in which maternal serum levels were retrospectively modeled. PFOA was associated with decreased birth weight in most of the studies from the general population but not in the study of the more highly exposed community. Inclusion of this study from the C8 Health Study population, in which serum PFOA levels during pregnancy were modeled from pre-pregnancy serum PFOA data and thus would not be impacted by potential changes in GFR, reduced the magnitude of decreased birth weight per ng/ml serum PFOA.
Several other reviews also evaluated the associations of PFOA and PFOS with decreased fetal growth. Bach et al. (2015) concluded that PFOA and PFOS are associated with decreased birth weight in most studies, but that associations in some studies were not statistically significant, and that the existing information is insufficient to determine whether or not there is an association. Khalil (2015) concluded that there is inconsistent evidence for association of decreased birth weight and PFAS. A later meta-analysis by Negri et al. (2017), which included more recent studies not considered by Johnson et al. (2014), also reported a quantitative relationship between decreased birth weight and serum PFOA and PFOS levels. A recent meta-analysis by Steenland, Barry, and Savitz (2018) considered additional studies not included in the two earlier meta-analyses, including the large studies from the C8 Health Study in which serum PFOA levels during pregnancy were modeled from pre-pregnancy serum PFOA data. Although Johnson et al. (2014) concluded that results from studies without measured serum data during pregnancy are too uncertain to include in a metanalysis, Steenland, Barry, and Savitz (2018) concluded that use of modeled or pre-pregnancy serum data may actually be preferable to serum levels measured during pregnancy because these exposure estimates would not be affected by potential reverse causality or confounding related to expansion of maternal plasma volume during pregnancy or renal glomerular filtration rate. Additionally, Steenland, Barry, and Savitz (2018) concluded that the decrease in birth weight in studies based on late pregnancy serum PFOA levels was larger than in those based on preconception or early pregnancy serum PFOA levels. They concluded that these findings are consistent with confounding or reverse causality as an explanation for the observed association of PFOA and decreased birth weight. A systematic review and modeling effort by Verner et al. (2015) found that PFOA is associated with decreased birth weight, and that a portion (less than half) of the reduction in birth weight results from confounding by associations of PFAS with decreases in both birth weight and maternal renal glomerular filtration rate (that is, reverse causality). USEPA (2023, 2023) concluded that there is general consistency in associations of PFOA and PFOS with decreased fetal growth, including low birthweight/small for gestational age. However, they noted uncertainties about the potential bias due to impact of changes in maternal hemodynamics, which may impact both serum PFAS levels and fetal growth, in the studies in which serum PFAS levels were evaluated later in pregnancy. The USEPA (2023) also concluded that PFDA is a likely developmental hazard based on evidence of decreased birth weight from studies of exposed humans where PFDA was measured during pregnancy.
ATSDR (2021), p.27, concluded that “evidence is suggestive of an association between serum PFOA and PFOS and small decreases in birth weight; the decrease in birth weight is <20 g (0.7 ounces) per 1 ng/mL increase in blood PFOA or PFOS level.” NASEM (2022) concluded that there is sufficient evidence for an association of PFAS with decreased infant and fetal growth. Australia Government DOH (2018) concluded that PFAS exposure was often associated with generally small decreases in weight and length at birth in general population studies. Steenland et al. (2020) reviewed the factors considered in evaluation of epidemiologic studies of PFAS and birthweight that are discussed above and concluded that collectively, the studies of PFOA and birthweight that are currently available provide inconsistent results.
Immune System Effects
Of the several potential effects of PFAS on immune function, the discussion below focuses on associations with antibody response to vaccines, including in children, because this endpoint has been evaluated and reviewed most extensively. A systematic review by the National Toxicology Program (NTP 2016), p.1, concluded that PFOA and PFOS are “presumed to be an immune hazard to humans” based on a high level of evidence from animal studies and a moderate level of evidence from human studies for suppression of antibody response. ATSDR (2021), p.27, concluded that “evidence is suggestive of an association between serum PFOA, PFOS, PFHxS, and PFDeA (meaning PFDA) levels and decreased antibody responses to vaccines.” For PFOA, PFOS, PFHxS and PFDA, the USEPA (2023) identified decreased antibody response to vaccination in children as an effect of exposure to these PFAS. Rappazzo, Coffman, and Hines (2017) found that there is generally consistent evidence for association of PFAS with this effect in children. NJDWQI (2017, 2018) concluded for PFOA that associations and decreased vaccine response are consistent among studies, and for PFOA, while decreased vaccine response was consistently observed, evidence is limited because most of the vaccine types were evaluated in only one or two studies. Pachkowski, Post, and Stern (2019) concluded that there is evidence that PFOS is associated with a decrease in some vaccine antibody responses following vaccination. Chang et al. (2016) concluded that a consistent association with vaccine response in general has not been demonstrated for PFOA and PFOS, and that some associations for specific vaccines are “striking in magnitude” but require replication in other studies. Australia Government DOH (2018), p. 11, concluded, based on review of key reports and systematic reviews, that “the strongest evidence for a link between PFAS and clinically important immunological effects is for impaired vaccine response.” They note both that the overall human evidence is weak, but that animal data suggests that “PFAS may alter immune function at concentrations found in humans with environmental and occupational exposures.” Khalil (2015) stated that PFAS exposure has been associated with immunotoxicity, including decreased vaccine response, but that the data are inconsistent. NASEM (2022) concluded that there is sufficient evidence for an association of PFAS with decreased antibody response in adults and children. USEPA (2023, 2023) concluded that PFOA and PFOS are associated with decreased antibody response to vaccines in children and concluded that the dose-response for each of these two PFAS can be modeled from the available human studies.
The C8 Science Panel concluded in 2012 that there was not a probable link between PFOA and common infections. Steenland et al. (2020) noted that there was insufficient evidence to infer such a probable link at that time, and that subsequent human and animal studies have evaluated the potential for PFOA to cause immunosuppression (for example, decreased vaccine response, increased infection) and hypersensitivity (for example, asthma, allergy). They reviewed the conclusions of several agencies (NTP 2016; ATSDR 2018 draft; EFSA 2018) and other available reviews regarding the evidence for immune system effects of PFOA, as well as recent studies that are relevant to this topic. The overall conclusion made by Steenland et al. (2020) was that “a relatively large number of studies consistently report that PFOA impairs immune function,” but that “evidence that PFOA increases the risk of infectious disease or asthma is inconsistent.”
Thyroid Effects
Evaluations of PFAAs and thyroid disease have reached varying conclusions. Although stating that the overall database was mixed, the C8 Science Panel determined a “probable link” for PFOA and thyroid disease (C8 Science Panel 2012). (NJDWQI 2017, 2018) found limited evidence for association of PFOA and thyroid disease, while associations of PFOS with thyroid disease were not noted, and Khalil (2015) found that the data for PFAS in general are inconsistent. Australia Government DOH (2018) concluded that “there are no consistent associations between any particular PFAS and thyroid hormones,” and that there is limited evidence of an association between PFOA and thyroid disease in women but not in men. Rappazzo, Coffman, and Hines (2017) stated that conclusions about PFAS and thyroid disease in children cannot be reached with certainty due to the small number of studies and variable results. Coperchini et al. (2017) found that hypothyroidism was the most consistent thyroid effect for PFOA, and for PFOS to a lesser extent, with women and children most susceptible. Ballesteros et al. (2017) stated that although there is a small number of studies with comparable data, there is some consistency in evidence for increased thyroid-stimulating hormone (TSH) with PFHxS and PFOS in pregnant women, and with PFNA TSH in teenage boys; associations with thyroid disease were not noted. More recently, a very large study (n = ~ 63,000) evaluated thyroid diseases in a Swedish community in which one-third of the population had previous residential exposure to very high levels of PFOS (8,000 ng/L) and PFHxS (17,000 ng/L) in drinking water. (Andersson et al. 2019). A consistent pattern of increased risk of hypothyroidism or hyperthyroidism was not found in men or women with residential exposure to the contaminated water. Steenland et al. (2020) concluded that there is less evidence for an association of PFOA and thyroid disease than when the “probable link” conclusion for this effect was made, and that studies of PFOA and thyroid hormone levels report inconsistent results. Similarly, ATSDR (2021), p.264, concluded that associations between PFOA, PFOS, PFHxS, PFNA, PFDA, and PFUnA and thyroid-related hormones and thyroid disease are inconsistent across studies, with the majority of studies not finding associations, and that most of the small number of studies of PFDoDA and thyroid hormones did not find “consistent associations.” NASEM (2022) concluded that there is limited or suggestive evidence for an association of PFAS with thyroid disease and dysfunction in adults and children. USEPA (2023) did not prioritize PFOA and thyroid disease as one of the key endpoints for evaluation of epidemiological associations. For PFOS, USEPA (2023) concluded that there is “slight evidence to suggest human endocrine toxicity, including associations between PFOS exposure and thyroid disease,” and that this conclusion is based on only one study rated as being of high confidence.
Other Effects
The C8 Science Panel also found probable links for PFOA with ulcerative colitis (C8 Science Panel 2012) and pregnancy-induced hypertension [PIH] (C8 Science Panel 2012); PIH was also associated with PFOS in the same two studies that linked it with PFOA (Stein, Savitz, and Dougan 2009; Darrow, Stein, and Steenland 2013). ATSDR (2021), p.26, concluded that “there is suggestive epidemiological evidence for an association between serum PFOA and PFOS and [PIH] and/or pre-eclampsia.” In the opinion of Steenland et al. (2020), current evidence continues to support a link of PFOA and ulcerative colitis, although more research is needed for a definitive conclusion, and NASEM (2022) concluded that there is limited or suggestive evidence for association of PFAS and this effect in adults. For pregnancy-induced hypertension, Steenland et al. (2020) reported mixed results; one recent study found an association with preeclampsia, a related effect, while another did not, and NASEM (2022) concluded that there is limited or suggestive evidence for association of PFAS and these effects.
For many other epidemiological endpoints that have been studied, generally consistent associations were not found and/or the available data are too limited to make firm conclusions.
It is notable that associations for several of the effects mentioned above (serum lipids, liver enzymes, vaccine response, birth weight) were observed even within the exposure range prevalent in the general population (without specific exposures from environmental sources), as well as at higher exposures. For several of these effects (for example, cholesterol—Steenland et al. 2009; Frisbee et al. 2010; ALT—Gallo et al. 2012), the dose-response curves (for example, serum lipids, liver enzymes) are steepest at very low exposures with a much flatter slope approaching a plateau at relatively low serum concentrations (for example, ~40 ng/L for PFOA and cholesterol).
17.2.4.2 Carcinogenicity
Several evaluations of the epidemiological evidence for carcinogenicity are available for PFOA and PFOS, while such evaluations have not been conducted for other PFAAs. The C8 Science Panel (2012) found a “probable link” of PFOA with testicular and kidney cancer based on an increased incidence of these cancers in the Ohio and West Virginia communities with drinking water exposure as well as data from other human and animal studies. Although some other occupational studies of PFOA, such as Raleigh et al. (2014), did not find increased incidence of these tumors, increased kidney cancer was reported in workers exposed to PFOA in the West Virginia industrial facility (Steenland and Woskie 2012). In consideration of these findings, IARC (2016) classified PFOA as “possibly carcinogenic to humans” (Group 2B) based on limited evidence that PFOA causes testicular and renal cancer, and limited evidence in experimental animals. Based on reviews of key reports and systematic reviews, the Australia Government DOH (2018), p.70, concluded that “the evidence on cancer risk is limited;” that it is possible that PFOA is associated with an increased risk of kidney and testicular cancer; and that the evidence does not support PFAS being a major contributor to cancer burden in workers or exposed community populations.
A recent study by the National Cancer Institute (Shearer et al. 2021) evaluated associations of serum concentrations of PFOA and other PFAS with renal cell cancer in a subset of participants in a much larger ongoing cancer screening trial. The analysis included 324 subjects diagnosed with renal cell cancer and 324 individually matched controls. PFAS were measured in blood samples taken prior to cancer diagnosis, and serum PFOA concentrations were within the range that was prevalent in the general population at the time of sample collection (1993–2001). Increased serum PFOA was associated with increased risk of renal cell cancer. This association remained even when subjects with decreased kidney function were excluded, and when only subjects with serum PFAS levels measured > 8 years before cancer diagnosis were included. Associations of serum PFOS and PFHxS with increased renal cell cancer risk were not statistically significant after adjustment for the other PFAS, while the association of increased risk with PFOA remained after this adjustment. The authors concluded that these results “add substantially to the weight of evidence that PFOA is a renal carcinogen and may have important public health implications.”
Steenland et al. (2020) concluded that the evidence for an association of PFOA and kidney and testicular cancer remains “supportive but not definitive.” They stated that although the results of three newer studies (published since the C8 Panel’s reports) are not consistent, the evidence for an association of PFOA with kidney cancer is strengthened by positive findings in the recent large case-control study in the general population (Shearer et al 2021).
NJDWQI (2017)–PFOA, NJDWQI (2018)–PFOS, concluded that PFOA and PFOS have suggestive evidence for human carcinogenicity, based primarily on animal data, while a more recent evaluation (NJDWQI 2023) concluded that current evidence for PFOA indicates that it is a likely human carcinogen. USEPA (2023) concluded that PFOA is a likely human carcinogen, citing recent animal (NTP 2020) and human (Shearer et al. 2021) studies that add support to earlier evidence of carcinogenicity. USEPA (2023) also concluded that PFOS is a likely human carcinogen, with a determination of a statistically significant trend for increased pancreatic acinar carcinomas in the chronic rat study (Thomford 2002; Butenhoff et al. 2012) adding support to earlier evidence. USEPA (2018) also concluded that GenX has suggestive evidence for human carcinogenicity. NASEM (2022) concluded that there is sufficient evidence for an association of PFAS and kidney cancer in adults and that there is limited or suggestive evidence for PFAS and breast and testicular cancer in adults.
In contrast to PFOA, studies of cancer incidence in large populations with exposure to contaminated drinking water with elevated levels of only PFOS are not available although a recent study evaluated communities with exposure to drinking water contaminated with PFOA, PFOS, and PFHxS (present at the highest concentration) from AFFF (Li et al. 2022). Arrieta-Cortes et al. (2017) concluded that while associations with cancer were not observed in the available occupational and general population studies of PFOS, such associations cannot be ruled out because problems with the studies may have precluded detection of associations if they were present. They therefore concluded that there is “inadequate evidence of carcinogenicity” based on the human data. Chang et al. (2014) stated that “many positive associations with PFOA exposure were detected in community settings” but were not confirmed in studies of workers with much higher exposures, although increases in certain cancers in some occupational studies are noted within the paper. They concluded that a causal association between PFOA or PFOS and human cancer is not supported by the currently available epidemiological evidence.
17.2.5 Animal Toxicology Studies
Many scientific considerations and decision points are involved in developing human health toxicity factors from animal toxicology data. In the hazard identification component of the toxicity factor development, the toxicological endpoint selected as the basis for the reference dose should be determined to be well established (that is, supported by multiple studies), related to an adverse health outcome, and relevant to humans based on mode of action considerations.
Peroxisome proliferator-activated receptor-α (PPAR-α) is a nuclear receptor found in many human and animal tissues that is involved with numerous physiological processes (Corton, Anderson, and Stauber 2000; Michalik et al. 2006). The role of PPAR-α in the effects caused by PFAS and the human relevance of effects in rodents that are mediated by PPAR-α have been a focus of research on the mode of action for the toxicological effects of PFAAs (Lau 2012; Post, Gleason, and Cooper 2017). As reviewed by Post, Gleason, and Cooper (2017), most PFAAs that have been evaluated for this effect can activate PPAR-α to some extent. Specific toxic effects of some PFAAs in rodent models occur wholly or partially via PPAR-α, while other effects are independent of PPAR-α. One important example is hepatic toxicity of PFAAs. For PFOS, hepatic effects are clearly primarily PPAR-α independent, while hepatic effects of PFOA and PFNA involve substantial contributions from both PPAR-α dependent and independent processes.
In the dose-response evaluation portion of toxicity factor development, the selected endpoint must provide the data needed to determine a point of departure (that is, benchmark dose [BMD], NOAEL, or LOAEL). To appropriately account for the large differences in PFAA half-lives among species, and among sexes of the same species in some cases, dose-response evaluation for long-chain PFAAs is most appropriately based on internal dose, as indicated by serum level, rather than external (administered) dose. Finally, in development of RfDs, uncertainty factors appropriate to the specific study and endpoint are selected and applied to the point of departure to account for factors such as sensitive human subpopulations, interspecies differences, shorter-than-chronic exposure duration, extrapolation from a NOAEL to a LOAEL, and potentially more sensitive toxicological effects (Section 8.3).
Toxicological effects that have been reported as statistically significant in mammalian laboratory animal studies for each PFAS, with relevant citations, are presented in the Table 17-8 Toxicological Effects Excel file. The sections following the table present general discussions of systemic, reproductive and developmental, and carcinogenic effects of these PFAS.
17.2.5.1 Systemic Effects
All of the PFAS included in the Table 17-8 Toxicological Effects Excel file for which data are available caused increased liver weight in the rodent and nonhuman primate species studied. For most of these PFAS, increased liver weight was accompanied by hepatocellular hypertrophy. Developmental (in utero or lactational) exposures to some PFAAs caused increased liver weight in rodent offspring. Many PFCAs, as well as PFOS and GenX, caused additional hepatic effects that are more severe in nature such as hepatocellular necrosis and/or vacuolation in rodents and nonhuman primates, or hepatic lipid accumulation in rodents. For PFOA (Butenhoff et al. 2012; NJDWQI 2017) and PFOS (Butenhoff et al. 2012; NJDWQI 2018), these hepatic effects increased in severity with longer duration of exposure and may represent a progression to neoplastic changes, including hepatic adenomas. Additional effects reported for some PFAS include bile duct toxicity in rodents and increased serum levels of liver enzymes in rodents and/or nonhuman primates.
Some PFAAs and PFECAs caused decreased serum cholesterol in rodents and/or nonhuman primates. The increased cholesterol in humans associated with much lower exposures to some PFAS may be attributable to interspecies differences, such as differences in activity of relevant receptors involved with cholesterol metabolism. However, these contrasting observations in rodents and humans may also arise from differences in the fat content of a typical low-fat laboratory diet and the higher fat diet in the humans who were studied (Tan et al. 2013; Rebholz et al. 2016), or to dose-related differences in this response, because the doses in the toxicology studies are much higher than human exposure levels.
Some long-chain PFAAs caused immune system toxicity in the (Table 17-8 Toxicological Effects Excel file. Decreased antibody response to antigens has been identified as a sensitive endpoint for PFOA and PFOS toxicity, and this endpoint in animal studies have been used as the basis for toxicity factors and health-based regulatory criteria developed by government agencies, including MDH (2019); ATSDR (2021); NJDWQI (2018); Pachkowski, Post, and Stern (2019).
The majority of PFAS covered herein have not been tested for neurobehavioral effects. Of those PFAAs that have been evaluated in rodents, exposure-related effects were not observed for PFBA and PFHxA, while exposure of adult rodents to PFOS and PFDA caused effects including changes in learning, memory, activity, and habituation or other effects indicative of cognitive defects (see studies cited in the Table 17-8 Toxicological Effects Excel file). Additionally, developmental exposures to PFOA, PFOS, and PFHxS caused persistent neurobehavioral effects in mice (Johansson, Eriksson, and Viberg 2009; Onishchenko et al. 2011; Lee and Viberg 2013).
17.2.5.2 Reproductive and Developmental
Reproductive effects in males and females and developmental effects of several PFAS have been evaluated in rodents (Table 17-8 Toxicological Effects Excel file), but these effects have not been studied in nonhuman primates. In addition to the considerations common to developmental toxicity studies in general, the much faster excretion of several PFAS in female rats than in males must be considered when interpreting results of the rat reproductive and developmental studies.
Dosing of pregnant females with PFAAs results in gestational exposure to the fetus and also to the offspring during lactation. Cross-fostering studies of PFOA (White et al. 2009) and PFOS (Luebker et al. 2005) in which dosed dams fostered pups from control dams and vice versa showed that effects such as delayed development can result from exposures during either gestation or lactation.
Although malformations have been reported in a few rodent studies of PFOA and PFOS, effects such as full litter resorptions, decreased litter or number of live pups at birth, decreased survival of neonates, and decreased fetal and neonatal weight have been more frequently and consistently found (USEPA 2023, 2023). These developmental effects may result from toxicity to the placenta, as has been observed for PFOA (Suh et al. 2011) and PFOS (Lee et al. 2015). With PFOS at relatively high doses, neonatal mice and rats appeared normal at birth but died within a few hours; the genesis of this phenomenon is not understood (multiple studies reviewed in NJDWQI 2018).
Decreased growth of offspring and/or delays in reaching developmental milestones was observed for several PFAS in rodent studies (Table 17-8 Toxicological Effects Excel file). For PFBS (Feng et al. 2017) and PFNA (Das et al. 2015), body weight decrements persisted until adulthood. PFOA caused delays in ossification of bones and eruption of teeth (Lau et al. 2006; Yahia et al. 2010). Developmental markers such as eye opening and/or reaching sexual maturity were also delayed by some PFAAs, while noting that sexual maturity was conversely accelerated in male mice by PFOA (Lau et al. 2006). Persistent neurobehavioral effects in mice resulted from developmental exposures to several long-chain PFAS (Johansson, Eriksson, and Viberg 2009; Onishchenko et al. 2011; Lee and Viberg 2013).
Certain developmental effects of some PFAAs persisted into adulthood. These include decreased size of uterus and ovaries, accompanied by decreased number of follicles and corpora lutea, and changes in reproductive and thyroid hormone levels in female mouse offspring exposed to PFBS (Feng et al. 2017). Developmental exposures of mice to PFOA caused persistent delays in mammary gland development (White et al. 2009) and persistent liver toxicity (Quist et al. 2015) at doses lower than those that caused other systemic and developmental effects; these endpoints have not been evaluated for other PFAS.
17.2.5.3 Chronic Toxicity and Tumorigenicity
PFAAs have generally not been found to be mutagenic or genotoxic (Lau 2015). Of the PFAS included in Table 17-8 Toxicological Effects Excel file, chronic studies that evaluated carcinogenicity and other effects of long-term exposure have been conducted in rats only for PFHxA, PFOA (three studies; one in males only), PFOS, and GenX. PFHxA did not increase the incidence of tumors in either sex of rats. PFOA increased the incidence of several types of tumors, including testicular Leydig cell adenomas in two of the three studies, and hepatic adenomas and/or carcinomas and pancreatic acinar cell adenomas and/or carcinomas in two of the three studies, and uterine adenocarcinomas in one of the three studies. In the chronic PFOS study, pancreatic acinar carcinomas and benign tumors in other organs were increased, including hepatic adenomas in females, and thyroid follicular cell adenomas in males only in the high dose “recovery group” (dosed for the first year only and evaluated at the end of the 2-year study). GenX increased the incidence of both hepatocellular adenomas and carcinomas in females, and the incidence of combined pancreatic acinar cell adenomas and carcinomas and testicular Leydig cell adenomas in males.
IARC (2016) classified PFOA as “possibly carcinogenic to humans” (Group 2B) based on limited evidence that PFOA causes testicular and renal cancer, and limited evidence in experimental animals. IARC (2023) is currently reevaluating the classification of PFOA and evaluating PFOS for the first time. Based on the USEPA (2005) Guidelines for Carcinogen Risk Assessment, USEPA (2023, 2023, 2018) described PFOA and PFOS as likely human carcinogens, and GenX as having suggestive evidence for human carcinogenicity. A recent review by NJDWQI (2023) concurred with USEPA (2023) that PFOA is a likely human carcinogen; this review also concluded that PFOS has suggestive evidence but did not consider the USEPA (2023) evaluation that found a statistically significant trend for pancreatic acinar tumors in the chronic rat study (see Section 17.2.3.5). For PFOA, ATSDR (2018), draft concluded that the hepatic tumors are unlikely to be relevant to humans. In contrast, USEPA (2023) concluded that, in the “absence of definitive information supporting a single, scientifically justified mode of action (MOA) and “evidence supporting the potential for multiple plausible MOAs, … USEPA takes the health-protective approach and concludes that the hepatic tumors observed [in two chronic rat studies]… can be relevant to human health.” Human relevance was not discounted for the testicular and pancreatic tumors by either ATSDR (2018) or USEPA (2023). For PFOS, USEPA (2023) and NJDWQI (2018) did not discount human relevance of the hepatic tumors. NJDWQI (2017) developed cancer slope (potency) factors for PFOA based on the incidence of testicular Leydig cell tumors in rats, while the California EPA (CA OEHHA 2023) and USEPA (2023) slope factors are based on the incidence of kidney cancer in humans and are much more stringent than PFOA slope factors based on animal data. NJDWQI (2018) and USEPA (2023)) both developed cancer slope factors for PFOS based on the incidence of liver tumors in rats.
17.2.6 Health Effects Information for Some Additional PFAS of Current Interest
17.2.6.1 Information Relevant to Human Health Effects of Ether and Polyether PFAS
There is increasing awareness and interest in potential human exposure to PFAS other than PFAAs. These include ether and polyether PFAS and dicarboxylic acid polyether PFAS used as replacements for long-chain PFAAs. Additionally, ether and polyether PFAS and PFAS with other structures can be formed as unintentional byproducts of industrial processes (Wang et al. 2019). Health effects information for hexafluoropropylene oxide dimer acid (HFPO-DA, GenX), a 6-carbon perfluoroether, and ADONA, a 7-carbon polyfluoropolyether, which are both used as replacements for PFOA, is discussed in Sections 7.1.4 and 17.2.5. Information on the environmental occurrence, ecological effects, toxicology and toxicokinetics in laboratory animals, and bioaccumulation and potential health effects in humans is currently becoming available for additional non-PFAA PFAS at a rapid pace, particularly for additional ether and polyether PFAS (Wang et al. 2019). Collectively, this information indicates that the toxicological and bioaccumulative properties of some of these ether and polyether PFAS, particularly those with longer total chain lengths (carbons plus ether oxygens in the chain), are similar to those of the phased out long-chain PFAAs (for example, PFOA, PFOS, PFNA) (see Figure 2-4).
This section summarizes the currently available laboratory animal and human studies that are relevant to human health effects of some additional ether and polyether PFAS. This material expands the discussion of these groups of compounds beyond HFPO-DA (GenX) and ADONA that were discussed in Section 17.2.5. These additional ether and polyether PFAS include:
- per- and polyfluoroether carboxylates (PFECAs)
- per- and polyfluoropolyether carboxylates (PFPECAs)
- per- and polyfluoroether sulfonates (PFESAs)
- per- and polyfluoropolyether sulfonates (PFPESAs)
As discussed below, some of the most thoroughly studied PFESAs and PFPECAs have chlorine atoms on the terminal carbon (ClPFESAs and ClPFPECAs, respectively). Toxicity data for dicarboxylic acid PFPECAs are also discussed. Specifically, longer chain PFPECA analogues of GenX (HFPO-DA), including hexafluoropropylene oxide-trimer acid (HFPO-TA) and hexafluoropropylene oxide-tetramer acid (HFPO-TeA), and numerous other PFPECAs of various structures and chain lengths are of interest because they are used as replacements for phased-out long-chain PFAAs and/or formed as industrial byproducts. Many of these PFPECAs have been detected in the environment, including in drinking water in some cases (Pan et al. 2019; Munoz et al. 2019; Wang et al. 2019; Kotlarz et al. 2020). Industrial mixtures of ClPFPECAs of various chain lengths, as well as dicarboxylic acid polyether PFPECAs, are also of interest because they are used as alternatives for phased-out long-chain PFCAs, including PFNA (NJDEP 2021; Wang et al. 2013), and ClPFPECAs have been detected in environmental media near industrial sources (McCord et al. 2020; Washington et al. 2020; Mazzoni et al. 2015).
F53B is a PFOS alternative that consists primarily of 6:2 chlorinated polyfluoroether sulfonate (6:2 ClPFESA), with smaller proportions of 8:2- and longer chain ClPFESAs (Munoz et al. 2019; see also Section 2.6.1.3). These ClPFESAs are used primarily in China, and are of interest because they have been found in multiple environmental media and, as discussed below, in human biomonitoring studies. Nafion byproducts are PFPESAs formed as industrial byproducts in the production of Nafion, a sulfonated tetrafluoroethylene-based fluoropolymer-copolymer, and are of interest because they have been found in drinking water impacted by industrial discharges (Hopkins et al. 2018). With some exceptions, the toxicity and bioaccumulative potential of PFAAs with similar structures (for example, PFCAs, PFSAs) generally increase with increasing carbon chain length (see Section 7.1.4). Similarly, currently available information on the ether and polyether PFAS with analogous structures (for example, HFPO-DA, -TA, -TeA; 6:2 and 8:2 ClPFESA) discussed in this section suggests that their toxicity and bioaccumulation also generally increase with increasing chain length (including both carbons and ether oxygens).
Human Biomonitoring and Health Effects Studies
PFECAs and PFPECAs
As discussed below, recent biomonitoring studies show that, as is the case for long-chain PFAAs, many ether and polyether PFAS are bioaccumulative in humans, although this may not be the case for some shorter chain members of this group such as GenX (HFPO-DA). Associations with changes in health-related endpoints (for example, clinical chemistry parameters) were also reported in some studies.
A biomonitoring study of Wilmington, NC, residents evaluated blood serum PFAS levels 5 months after cessation of exposure to drinking water from the Cape Fear River that was contaminated by multiple PFAS. Nafion byproduct 2 and two longer chain PFPECAs were detected in the blood serum of >85% of subjects; two other fluoroethers were less frequently detected. The shorter chain PFECA, GenX (HFPO-DA), which was also present in drinking water, and several other PFAS that were detected in the Cape Fear River, were not found in human serum (Kotlarz et al. 2020). This study did not evaluate potential associations of health effects and exposure to fluoroethers. Yao et al. (2020), whose study population lived near a fluorochemical plant in China, also detected multiple PFECAs and PFPECAs, as well as sulfonate ether PFAS (discussed below), in blood serum. They reported associations between PFO5DoA, a long-chain PFPECA that has 7 carbons and 5 ether oxygens, and increased serum lipids, liver enzymes, and uric acid. Two other PFECAs (HFPO-TA, 9 carbons and 2 ether oxygens; PFO4DA, 6 carbons and 4 ether oxygens) were associated with increases in one or more serum lipid parameters, and PFO4DA was also associated with increased uric acid.
A summary of an unpublished biomonitoring study of workers with occupational exposure to industrial mixtures of ClPFPECA congeners of various chain lengths reported an estimated human half-life of 2.5–3 years. Associations with increased serum lipids, liver enzymes, triglycerides, albumin, albumin/globulin ratio, thyroid stimulating hormone (TSH), free thyroxine, and prostate-specific antigen (PSA), and decreases in estradiol and indicators of immune system function (alpha-2-globulins and immunoglobulins) were reported (Solvay 2019). It was noted that the changes in serum lipids and liver enzymes may have been confounded by exposure to PFOA, and that associations with increased TSH and PSA were less reliable because they were based on fewer data points (Solvay 2019).
PFESAs and PFPECAs
6:2 ClPFESA was consistently detected in human blood serum in several recent biomonitoring studies in China (Jin et al. 2020; Liu et al. 2020; Pan et al. 2017; Yao et al. 2020). The median and mean human half-life of 6:2 ClPFESA were estimated as 15.3 and 18.5 years, respectively, as compared to an estimated median and mean of 6.7 and 7.7 years, respectively, for PFOS in the same study (Shi et al. 2016). 6:2 ClPFPESA was included in the suite of PFAS measured in blood serum of U.S residents in NHANES for the first time in 2017–18 (CDC 2022). It was found at the detection limit (0.100 ng/ml) in the 95th percentile of the total population, and at the same or similar levels in most racial/ethnic groups as follows: Mexican Americans – not detected at 90th percentile, 0.100 at 95th percentile; non-Hispanic blacks – 0.100 ng/ml at 90th and 95th percentiles; non-Hispanic whites – not detected at 95th percentile; all Hispanics – not detected at 90th percentile, 0.100 at 95th percentile [values are geometric means]. The maximum level detected in any of these subgroups was 0.200 ng/ml. However, it was detected more frequently and at higher levels in Asians (0.200 ng/ml at 75th percentile; 1.00 ng/ml at 90th percentile; 2.30 ng/ml at 95th percentile; maximum – 10.9 ng/ml). It is not known whether the more frequent detections and higher serum levels in Asians results from their exposure while in Asia or from other sources such as consumption of foods contaminated with 6:2 ClPFESA that are imported from Asia.
As is the case for long-chain PFAAs, biomonitoring data demonstrate exposure to ClPFESAs in utero and through breast milk. Both 6:2 and 8:2 ClPFESA were found in matched maternal:umbilical cord blood samples, indicating fetal exposure, with 8:2 ClPFESA having a higher rate of transfer to cord blood (Cai et al. 2020; Chen et al. 2017; Pan et al. 2017; Xu et al. 2019). The only study that evaluated potential health outcomes associated with fetal exposure found no evidence of an association between ClPFPESAs exposure and birth outcomes (Xu et al. 2019). 6:2 and 8:2 PFESA were also found in human breast milk from several locations in China, but not from Sweden (Awad et al. 2020; Jin et al. 2020). Breast milk levels of these PFESAs were associated with decreased infant growth in one of these studies (Jin et al. 2020).
Rodent Toxicology Studies
PFECAs and PFPECAs
As discussed above, hepatotoxicity is an effect common to many PFAS. In mouse studies, HFPO-TeA, with 12 carbons and 3 ether oxygens, was more hepatotoxic than its shorter chain analogue HFPO-DA (GenX; Wang et al. 2017), and HFPO-TA, with 9 carbons and 2 ether oxygens, was more hepatotoxic than PFOA, which has an 8-carbon chain (Sheng et al. 2018). In mice, the bioaccumulation in blood serum and liver increased with chain length for a series of PFPECAs with two to four O-CF2 groups, and only the largest PFAS, with four such groups (PFO4DA), caused increased liver weight at the doses tested (Guo et al. 2019). A recent study (Chen et al. 2021) reported half-lives in male mice of 24 hours for PFO4DA and 43 days for its larger homologue, PFO5DoA after a single intravenous dose. In a 140-day study of male mice, both compounds accumulated in the liver and caused increases in body weight, relative liver weight, and serum glucose, triglycerides and free fatty acids, as well as biochemical changes in the liver consistent with reduced glycolysis (Chen et al. 2021).
As reviewed in NJDEP 2021, industrial products consisting of mixtures of ClPFPECA congeners of various chain lengths ranging from 8 carbons and 3 ether oxygens to 14 or 17 carbons and 5 ether oxygens caused toxicity to liver, lung, thymus, seminal vesicles, and thyroid in 4-week and/or 13-week rat studies, with some changes persisting after a several-week recovery period (Research Toxicology Centre 2006, 2016). The doses at which hepatic effects occurred were similar to those reported for long chain PFCAs (for example, PFOA, PFNA; NJDWQI 2015, 2017). The half-lives for five of the congeners (ranging from 8 carbons and 3 ether oxygens to 14 carbons and 5 ether oxygens) were reported as 8–29 days in male rats and 1.6–91 days in female rats. These half-lives are similar to those documented for PFOA (4-6 days) and PFNA (30 days) in male rats (Table 17-7).
Additionally, industrial products consisting of mixtures of another type of PFPECAs, dicarboxylic acid polyether carboxylates (chain lengths not specified), caused toxicity to the liver, lung, thymus, seminal vesicles, and kidneys, with hepatic effects at very low doses, in 4- and/or 13-week studies in rats. As for the ClPFPFECAs, some effects persisted after a several week recovery period. The estimated half-life in male rats after a single dose was 43 days, and the estimated half-lives after repeated dosing were approximately 8 days in males and 11 days in females (Research Toxicology Centre, 2005; Research Toxicology Centre, 2006). In contrast, PFOA and PFNA, with half-lives of 2-4 hours and 1-2 days, respectively, as well as some other PFAS, are much less persistent in female rats (Section 17.2.3; Table 17-7).
PFESAs and PFPESAs
6:2 ClPFESA, the primary component of F53B, and Nafion byproduct 2, also a PFPESA, caused liver toxicity in mice (Zhang et al. 2018; Lang et al. 2020). In a subchronic study of reproductive toxicity of 6:2 ClPFESA in male mice, relative weights of reproductive organs decreased at the highest dose tested. However, at the doses used in the study, there were no histopathological changes in these organs, and hormone levels, sperm counts, fertility, and expression of several testicular genes were not affected (Zhou et al. 2018). After subchronic exposure to mice, 6:2 ClPFESA accumulated in the small and large intestine, damaged the gut barrier, and caused inflammation of the colon (Pan et al. 2019).
Zebrafish Studies
Zebrafish are well accepted as an in vivo model system for human health effects. Zebrafish studies for the ether and polyether PFAS are relevant to evaluation of their potential human health effects and are discussed below.
PFECAs and PFPECAs
The hexafluoropropyl acids—HFPO-DA, HFPO-TA, and HFPO-TeA—caused estrogenic effects in zebrafish (Xin et al. 2019). A suite of PFPECAs of various chain lengths decreased thyroid hormone levels in developing zebrafish embryos, leading to thyroid hormone-dependent malformations of the swim bladder (Wang et al. 2020).
6:2 ClPFECA
A number of studies have reported toxic effects of 6:2 ClPFECA in zebrafish. These include: bioaccumulation in larvae and adults (Wu et al. 2019); hepatoxicity, in adults (Shi et al. 2019; Wu et al. 2019); reproductive toxicity in a two-generation study (Shi et al. 2018); disruption of cardiac development (Shi et al. 2017); and thyroid toxicity from developmental exposures to environmentally relevant concentrations (Deng et al. 2018) and in unexposed offspring after exposure of the parental generation (Shi et al. 2019). Tu et al. (2019) reported that 6:2 ClPFECA was more bioaccumulative and was a more potent disruptor of metabolism than PFOA in zebrafish.
17.2.6.2 Fluorotelomer Alcohols
Fluorotelomer alcohols (FTOHs) are polyfluoroalkyl substances synthesized as intermediates for the manufacture of various fluorosurfactants and fluoropolymers (Dinglasan-Panlilio and Mabury 2006; ECHA 2012). The telomer alcohols are named with the number of fully fluorinated carbon atoms first, followed by the number of partially fluorinated carbon atoms (for example, 8:2 FTOH, 6:2 FTOH). In the environment, FTOHs may degrade to PFCAs with 8:2 FTOH degradation capable of forming PFOA and PFNA (Butt, Muir and Mabury 2014). FTOHs are present in multiple consumer products, with 6:2 FTOH the primary FTOH manufactured for end use. Humans may be exposed by ingestion of FTOH-contaminated food or dust (Yuan et al. 2016). Some FTOHs are volatile, and human exposure may also occur via inhalation (Huang et al. 2019).
The following section summarizes currently available information on the toxicokinetics and adverse health effects of 6:2 and 8:2 fluorotelomer alcohol (6:2 and 8:2 FTOH, respectively) in experimental animals and humans. No peer-reviewed data were identified for other FTOHs.
Toxicokinetics
As polyfluoroalkyl substances, FTOHs are extensively metabolized in rodents and humans. Depending on the specific FTOH, the terminal metabolites include long- and/or short-chain PFCAs, unsaturated fluorotelomer acids (FTUCAs), fluorotelomer acids (FTAs) and glutathione, sulfate, and glucuronide conjugates (Kudo et al. 2005; Fasano et al. 2006, 2009; Himmelstein et al. 2012; ECHA 2012; Nilsson et al. 2013; Kabadi et al. 2018; Huang et al. 2019; Rice et al. 2020).
6:2 FTOH is rapidly absorbed following oral exposure, and undergoes metabolism in rats to form PFBA, PFPeA, PFHxA, PFHpA, certain FTAs, and glutathione, sulfate, and glucuronide conjugates (Russell et al. 2015; Kabadi et al. 2018). In vitro metabolic data from hepatocyte cultures indicate that 6:2 FTOH is likely metabolized similarly in rat, mice, and humans (reviewed in Rice et al. 2020). One of the non-PFCA metabolites, 5:3 FTA, is persistent, having an estimated half-life of ~100 days in male and female rats after repeated dosing (Kabadi et al. 2020). Russell et al. (2015) calculated an apparent geometric mean elimination half-life of 43 days for 5:3 FTA in humans based on occupational data of Nilsson et al. (2010, 2010, 2013). PFHxA and the other terminally stable short-chain PFCAs formed by the metabolism of 6:2 FTOH do not undergo further degradation and are eliminated rapidly in rodents (see Table 17-7). The metabolic pathways, rate determining steps, and elimination half-lives of the parent 6:2 FTOH and other metabolites have not been established.
8:2 FTOH administered orally or by inhalation is also rapidly absorbed and metabolized in rats and mice, with PFOA, 7:3 FTA, 8:2 FTA, PFNA, PFHxA, PFHpA, and glucuronide, glutathione, and other conjugates identified as metabolites (Kudo et al. 2005; Fasano et al. 2006, 2009; Himmelstein et al. 2012; ECHA 2012). In vitro data from rat, mouse, and human hepatocytes indicate that 8:2 FTOH is metabolized to PFOA in rodents and humans, although rodent hepatocytes appear to transform greater amounts of 8:2 FTOH to PFOA than human hepatocytes. Other in vitro metabolites in rodent hepatocytes include 8:2 FTCA, 8:2 FTUCA, and PFNA (ECHA 2012).
Data from the NTP (Huang et al. 2019) confirmed that 8:2 FTOH is rapidly absorbed and distributed in male and female rats after a single oral or intravenous (IV) dose. The plasma elimination half-life of the parent compound was 1.1–1.7 hours, and the two primary metabolites were 7:3 FTA and PFOA. The half-life of 7:3 FTA was 2–3 days in both sexes of rats; PFOA’s half-life was sex-dependent (approximately 8–15 days in males, and 4.5–6.9 h in females). Nilsson et al. (2010, 2010) measured a mixture of 6:2, 8:2, and 10:2 FTOH and other PFAS in the workplace air of ski wax technicians and subsequently documented the presence of PFOA, PFNA, PFDA, PFDoA, PFTDA, 5:3 FTA, and 7:3 FTA in all samples of the technicians’ blood (Nilsson et al. 2013). The metabolites, 8:2 FTUCA and 10:2 FTUCA, were also detected in blood samples from multiple technicians. Although concentrations of 8:2 FTOH were several-fold higher than other PFAS in workplace air, the relative importance of 8:2 FTOH and 10:2 FTOH to the metabolic formation of PFOA, PFNA, other long-chain PFCAs, or the FTAs cannot be determined from these data given that exposures were to multiple PFAS.
Toxicity
6:2 FTOH
Consistent with other data that have demonstrated a lack of genetic toxicity of PFAS (see Section 17.2.5.3), 6:2 FTOH was negative when tested in the Ames bacterial mutagenesis assay. It was not mutagenic in the mouse lymphoma assay and was not clastogenic in a chromosome aberration assay in human lymphocytes. It was found not to be a skin or eye irritant (Serex et al. 2014).
Given the metabolic transformation of 6:2 FTOH and 8:2 FTOH to several PFCAs, 5:3 FTA (6:2 FTOH metabolite), and multiple additional metabolites of unknown toxicity, it is unclear whether adverse effects associated with exposure of experimental animals to FTOHs (see following) are attributable to the parent FTOH, one or more metabolites, or to combined exposure to multiple compounds. With the exception of the persistent 5:3 FTA metabolite of 6:2 FTOH, for which limited data demonstrating toxicity are available (Rice et al. 2020), the relationship between the adverse effects of FTOHs and their metabolites has not been established.
Rice et al. (2020) synthesized toxicity data on 6:2 FTOH from a 28-day NTP study, a number of peer-reviewed publications (Miyata et al. 2007; Kirkpatrick 2005; O’Connor et al. 2014; Serex et al. 2014; Mukerji et al. 2015), and OECD-compliant studies submitted on behalf of FTOH manufacturers. These studies reported that 6:2 FTOH causes multiple effects in the liver (for example, increased serum liver enzymes, hepatocellular necrosis, and oval cell hyperplasia) and kidney (renal tubular necrosis, mineralization, and degeneration) in rats and mice, as well as decreased thymus weight in rats. Reproductive effects of 6:2 FTOH in rats were observed only when high maternal mortality occurred. In contrast, 6:2 FTOH caused decreased body weight gain during lactation, mammary gland lesions, decreased uterine and ovarian weights, and an increase in anestrus in mice. 6:2 FTOH elicited developmental effects in both rats and mice, including increased pup mortality, delayed skull ossification, decreased pup body weight gain in rats, and decreased pup survival during lactation in mice.
Rice et al. (2020) also summarized the results of a 2-week oral toxicity study of the persistent 6:2 FTOH metabolite 5:3 FTA as reported by the industrial manufacturer. Those data indicate that in rats, 5:3 FTA caused adverse effects on the liver (decrease in total cholesterol, hepatocyte necrosis); kidney (increase in creatinine and urine volume, decrease in total urine protein); thyroid (follicular cell hyperplasia); and thymus (decrease in thymus weight).
There are no publicly available chronic toxicity studies for 6:2 FTOH.
8:2 FTOH
8:2 FTOH was negative when tested in the Ames bacterial mutagenicity study (NTP 2018), and in micronucleus assays reported by the OECD (ECHA 2012).
The liver and kidney were the primary target organs in rats administered 8:2 FTOH orally over a 90-day period (Ladics et al. 2008). 8:2 FTOH caused hepatic necrosis in males, and induced kidney nephropathy in females. Urinary and/or plasma fluorine levels were elevated in animals from all dose groups, an effect attributed to metabolism of the parent compound and an associated increase in fluoride levels. Wang et al. (2019) also documented effects of 8:2 FTOH on the livers of mice, including cellular vacuolation and swelling; swelling of cell nuclei; and immune cell infiltration in animals exposed orally for 28 days. 8:2 FTOH significantly altered mRNA levels of inflammatory cytokines in the thymus and spleen, although it is unclear whether these changes would translate to biologically significant effects on the immune system, as there were no accompanying histological changes in these organs.
Mylchreest et al. (2005) assessed the developmental toxicity of 8:2 FTOH in rats, finding that increased skeletal malformations in pups (delayed pelvic bone ossification and wavy ribs) occurred only at a dose that also elicited maternal toxicity. Mylchreest et al. (2005) also evaluated the reproductive and developmental toxicity of a commercial mixture of FTOH in rats, and observed decreases in litter size, pup weights, and the number of live pups per litter on days 0 and 4 of lactation. Developmental effects were seen only at a dose that also caused maternal toxicity.
There are no publicly available chronic toxicity studies for 8:2 FTOH.
17.2.6.3 Fluorotelomer Sulfonic Acids
Fluorotelomer sulfonic acids (FTSAs) and their salts, the fluorotelomer sulfonates (FTS), are polyfluorinated chemicals that are formed both by direct manufacture and by the degradation of precursors found in certain AFFFs or other industrial products (see Section 2.2.4.1; Field and Seow 2017). Because FTSAs and FTSs exist in anionic form in the body, they are equivalent toxicologically, and the term FTSA is used here to refer to both forms of these chemicals.
4:2 FTSA, 6:2 FTSA, and 8:2 FTSA have been detected in human blood (Lee and Mabury, 2011; Loi et al. 2013; Yeung and Mabry 2016; Eriksson et al. 2017), and 6:2 FTSA and 8:2 FTSA can cross the human placenta (Yang et al. 2016). Humans may potentially be exposed to FTSAs through ingestion of contaminated drinking water or food, or by inhalation of dust (Field and Seow 2017). It is not known if the detection of FTSAs in human blood is due to direct exposure to the parent compounds or to indirect exposure to FTSA or precursors (Field and Seow 2017).
Toxicokinetics
Information on the toxicokinetics of FTSAs is limited. No studies have evaluated the absorption of FTS versus FTSA. Since FTS and FTSA exist in the same anionic form within the body, their toxicokinetics would not differ after absorption. ECHA (2018) provided summary information on a single rodent in vivo study that examined the disposition and metabolism of 6:2 FTSA (species and dose levels not given). Following a single oral dose of 6:2 FTSA, 65–68% of the parent compound was recovered in urine 4 days post-dosing, indicating that metabolism of the majority of the administered dose did not occur. However, because no data were provided on metabolite formation or elimination, many questions remain regarding the metabolism of 6:2 FTSA in animals. In vitro data from ECHA (2018) and Hoke et al. (2015) also suggested that 6:2 FTSA is not extensively metabolized in animals. When 6:2 FTSA was incubated with rat liver microsomal fractions for 2 hours (ECHA 2018) or with rainbow trout hepatocytes for 4 hours (Hoke et al. 2015), no metabolism was detected. FTSA may have the potential to bioaccumulate, in that substantial levels of FTSA were measured in the livers of mice administered FTSA for 28 days (Sheng et al. 2017). The potential of FTSA to bioaccumulate is supported by observations of Yan et al. (2014), who found comparable levels of the bioaccumulative PFOA in the serum and livers of mice exposed under the same experimental conditions used for FTSA by Sheng et al. (2017). In the few human biomonitoring studies that included 6:2 FTSA, it was detected infrequently. For example, the Biomonitoring California Asian/Pacific Islander Community Exposures Project reported no detections of 6:2 FTSA in 2016 (N=96) and FTSA was detected in only 3% of samples analyzed in 2017 (N=99) (LOD=0.05 ng/ml) (CA OEHHA 2020).
Toxicity
6:2 FTSA was not genotoxic in assays of bacterial mutagenesis, or in mammalian cell assays of DNA repair or damage, micronucleus formation, or chromosome aberrations (ECHA 2018).
ECHA (2018) reported the results of unpublished oral range-finding and reproductive toxicity studies in rats. The 14-day range-finding study identified a NOAEL of 10 mg/kg-d based on changes in body and kidney weights and clinical chemistry (creatinine and urea) in one or more dose and gender groups. In the 90-day reproductive toxicity study, 6:2 FTSA did not affect male or female fertility or reproductive performance, and there were no effects on the number of pups, or on pup survival, growth, or sex ratio. The NOAEL for reproductive effects was > 45 mg/kg-d.
Adult male mice administered 6:2 FTSA at 5 mg/kg-d over 28 days exhibited increases in liver weight, hepatocellular hypertrophy, hepatocellular necrosis, and biochemical markers associated with liver inflammation. Serum levels of the liver enzyme AST, an indicator of liver damage, and albumin were also elevated, and histological evidence of liver necrosis was observed (Sheng et al. 2017).
Adult male and female mice administered were administered 6:2 FTS over 112 days. 6:2 FTS is the anionic form of 6:2 FTSA which dissociates into 6:2 FTS, as is described in Section 2.2.3.1. Male and female mice exhibited signs of immunotoxicity including decreased plaque-forming cells in the spleen in response to sheep red blood cells in males and females administered 5 and 25 mg/kg-d and increased spleen weight in males administered 5 mg/kg-d (Bohannon et al. 2023).
17.2.7 PFAS Mixtures
This section provides a brief overview of current toxicity-based approaches for addressing mixtures of PFAS and currently available information on toxicity of PFAS mixtures. This is an active area of research.
17.2.7.1 Proposed Approaches, for Addressing Toxicity of PFAS Mixtures
Total Concentration Approach (Called Simple Additive Approach by Cousins et al. 2020)
In this approach, a single guideline concentration is applied to the total concentration of a specified set of PFAS. This approach is based on the assumption that all of the included PFAS have the same toxic effects and MOA, are equally potent, and their combined toxicity is additive. In the absence of complete information on toxicity and MOA for all of the selected PFAS, this approach has been applied as a conservative public health-protective science-policy strategy.
Examples of this approach are the drinking water guidelines of 20 ng/L (Vermont) and 70 ng/L (Connecticut) for the total concentration of five long-chain PFAAs (PFOA, PFNA, PFHpA, PFOS, PFHxS) and 20 ng/L (Massachusetts) for the total concentration of six long-chain PFAAs (PFOA, PFNA, PFHpA, PFOS, PFHxS, PFDA) (CT DPH 2016; Vermont DOH 2018; MA DEP 2019), as well as in several other nations (Cousins et al. 2020).
MA DEP (2019) provided a detailed rationale for their approach based on the sum of the six long-chain PFAS. They concluded that this approach is supported by similarities in chemical structures, toxicity values developed by other agencies, toxicological responses, and long serum half-lives for these six PFAS. PFHxA was also considered but was not included, because it has a shorter half-life and causes toxicity at higher doses than the PFAS that were included.
MA DEP (2019) used results of Bayesian benchmark dose (BBMD) modeling of data for thyroid effects (free thyroxine; fT4) and increased liver weight for five of the six PFAS from NTP 28-day rat toxicology studies (NTP 2019). Using PFOA as an index compound with a BBMD of 1, relative BBMDs for fT4 for the other PFAS ranged from 0.5 to 3 on a serum-level basis and 0.8 to 4 on a human equivalent dose (HED) basis. For an increase in liver weight, relative BBMDs based on both serum PFAS levels or HEDs ranged from 0.2 to 2. MA DEP (2019) considered these BBMDs to be sufficiently similar to assume equivalence of the five PFAS.
As discussed by MA DEP (2019), there is a lack of data on toxicological effects, potency, and half-life of PFHpA (the 7-carbon PFAA included in the Connecticut, Vermont, and Massachusetts approaches), and no toxicity values (for example, reference doses) have been developed. Although Massachusetts recognized that PFHpA’s half-life is likely shorter than for PFOA, they concluded that there are no data to develop a compound-specific or relative toxicity value for PFHpA, or to conclude that it is toxicologically dissimilar to PFOA. Based on “read-across,” (prediction of toxicity based on data from similar compounds) these states consider PFHpA to be equipotent to PFOA.
Hazard Index Approach
Human health risk assessment often uses a hazard index approach, first developed by USEPA (1989), to evaluate the potential cumulative noncancer toxicity from co-exposure to multiple contaminants (USEPA 1989). As discussed in Section 9.1.3.1, calculation of a hazard index is based on the assumption of dose additivity, but it does not necessarily require that the MOA or toxicological endpoint is the same for all components of the mixture. As discussed in USEPA (2023), the Hazard Index approach can be based on a “general” Hazard Index, in which noncancer toxicity factors for multiple contaminants are used regardless of whether they are based on effects in the same or different target organs, or a “target organ specific” Hazard Index in which noncancer toxicity factors are based on effects in the same target organ. USEPA (2023) presented the basis for a proposed MCLG and MCL of a Hazard Index of 1 for mixtures of four PFAS (PFBS, PFHxS, PFNA, GenX). The draft MCLG and MCL use the “general” Hazard Index approach in which the Hazard Index considers toxicity values based on differing toxicological endpoints for evaluation of the toxicity of the mixture.
Health Canada (2018, 2018) has concluded that, although there are no in vivo studies of PFAS mixtures, the similarity in health effects of PFOA and PFOS support an assumption of dose additivity and thus support the use of a hazard index approach to address co-occurrence of PFOA and PFOS in drinking water. ATSDR has also applied the hazard index approach to evaluate potential risk from site-specific exposure to mixtures of several long-chain PFAAs, noting that their approach assumed dose additivity based on “toxicologic similarities” (ATSDR 2020).
Minnesota Department of Health (undated) uses a health risk index approach—similar to the target organ specific Hazard Index approach—to evaluate concurrent exposures to multiple chemicals in groundwater. It is based on grouping chemicals (including PFAS and others) that cause the same general type of adverse health effect (i.e., the same target organ—for example, thyroid, endocrine). In the Minnesota health risk index approach, multiple health endpoints may be considered for each individual contaminant.
Mumtaz et al. (2021) provided a “proof of concept” demonstration of the potential use of an ATSDR hazard index approach based on target organ toxicity doses (TTDs) for specific toxicological effects (endocrine, hepatic, reproductive, developmental, and/or immune) to assess the risks of PFOA, PFOS, tetrachlorodibenzo-p-dioxin (TCDD), and polybrominated diphenyl ethers (PBDEs). This approach is intended for use as a screening tool, with a hazard index of >1 for a specific effect indicating the need for further evaluation.
USEPA (2023) has recently proposed to regulate four PFAS (PFBS, PFHxS, PFNA, GenX) in drinking water based on the general Hazard Index approach.
Relative Potency Factor (RPF) Approach
In the RPF approach, each PFAS is assigned an RPF based on its potency compared to an index compound (for example, PFOA), which is assigned a potency factor of 1. The RPFs are applied to the concentration of each PFAS present in the mixture, and the toxicity of the total of the RPF-adjusted concentrations is assumed to be the same as the equivalent concentration of the index compound (for example, PFOA). See USEPA 2023 for more information about the RPF approach.
The RPF approach is based on dose additivity of the compounds that are included (see discussion in Hazard Index section above). The RPF approach (also known as the toxicity equivalency factor approach) has been adopted for several groups of chemicals known to cause toxicity through a common and well-defined MOA, including cholinesterase-inhibiting pesticides (organophosphates) and dioxins (PCDDs) and dioxin-like compounds (furans [PCDFs]; PCBs) that cause toxicity through activation of the AhR receptor.
The application of the RPF approach for risk assessment of PFAS mixtures is associated with greater uncertainty than for the groups of compounds noted in the preceding paragraph. In contrast to the groups of compounds discussed above, the range of adverse effects of PFAS is not due to a single specific MOA, such as activation of a specific receptor. Furthermore, the MOA may not be the same for all toxicological effects (for example, hepatic toxicity; developmental toxicity) and may vary among PFAS (discussed in this Mixtures section above).
Bil et al. (2021) proposed RPFs for 22 PFAS, with PFOA as the index compound. This is an extension of an earlier proposal of RPFs for 18 PFAS developed by RIVM (Netherlands National Institute for Public Health and the Environment) scientists (Zeilmaker et al. 2018). The RPFs were based on hepatic effects of PFOA and 15 other PFAS in male rats from studies with durations of 40–98 days. Hepatic effects in male rats were selected because these effects are common to many PFAS, and there is a large data set on these effects in male rats. Endpoints evaluated included relative liver weight (all 16 PFAS), absolute liver weight (15 PFAS), and hepatocellular hypertrophy (14 PFAS), and the final RPFs were based on relative liver weight because the data set was most complete. Relative liver weight data for all PFAS (based on external dose) were fit to parallel dose-response curves, which were determined to provide an acceptable fit to the data. BMDs for each PFAS for each effect were developed from the dose-response curves based on a 5% change in absolute or relative liver weight and a 10% change in the incidence of hepatocellular hypertrophy. RPFs were based on the ratio of the BMDs for each PFAS to the BMD for PFOA and ranged from 0.001 (PFBS) to 10 (PFNA). RPF ranges for seven additional PFAS for which no relevant data were available were estimated by read-across/interpolation.
In contrast, Peters and Gonzalez (2011) concluded that it is not appropriate to develop TEFs (similar to RPFs) for PFAS for reasons including differing modes of actions among PFAS. However, Bil et al. (2021) discussed that although the MOA for hepatic effects may differ among PFAS, the similarly shaped dose-response curves for these effects support the assumption of additivity and the application of RPFs for hepatic effects. They also note the need to determine whether the RPFs based on hepatic effects are applicable to other types of toxicity caused by PFAS, such as developmental and immune system effects—an analysis that has not yet been conducted. Goodrum et al. (2021) concluded that the shapes of the dose-response curves for hepatocellular hypertrophy for PFOS and PFHxS in male rats, based on administered dose, differ from the dose-response curves for this effect for other PFAAs. When based on internal dose (serum levels), the shape of the curve for PFHxS differed from the shape of the curves for the other long-chain PFAAs. These results suggest that PFHxS, and possibly PFOS, are not additive with other PFAAs for hepatocellular hypertrophy in male rats; curves for liver weight were not evaluated.
17.2.7.2 Toxicology Studies of Defined PFAS Mixtures
Only a few studies of the toxicity of mixtures of PFAS, including studies of defined mixtures (i.e., mixtures for which the identities and concentrations of the components are known) of PFAS and studies of complex mixtures (i.e., mixtures for which the identities and concentrations of the components are not fully characterized) of PFAS such as AFFF were located; these are summarized below. These include in vitro studies of nuclear receptor activation in cultured cells transfected with the receptor of interest, and toxicity in cultured cells, zebrafish (a model species for human toxicity), and rodents.
Mammalian Studies
Defined PFAS Mixtures
Several recent studies have evaluated effects of defined mixtures of PFAS in mammalian species. Marques et al. (2021) dosed pregnant mice fed either a standard lab diet or a high fat diet with 1 mg/kg/day PFOA, PFOS, or PFHxS, individually, or 1 mg/kg/day of all three PFAS, throughout gestation. The authors concluded that “the PFAS mixture had very distinct effects when compared to single compound treatment, suggesting cumulative properties of the mixture, particularly when evaluating PFAS transfer from dam to pup,” and that “these results suggest that there are multiple pathways in which PFAS could add, synergize, or antagonize specific effects, and warrants further investigation of dose response data with model predictions of additivity.” However, as noted by USEPA (2023), “these studies did not include individual PFAS dose response data or conduct any mixture model-based analyses, so it is not possible to ascertain if the mixtures behaved in a dose additive or risk additive manner, or if interactions occurred.”
Roth et al. (2021) evaluated the effects of exposure to a mixture of PFOA, PFOS, PFNA, PFHxS, and GenX (2 mg/L each) in drinking water in mice fed a high fat diet. This treatment increased serum cholesterol, sterol metabolites, and bile acids, and caused liver toxicity, with some differences between males and females. However, the toxicological interactions among PFAS in this study cannot be determined because effects of individual PFAS were not evaluated.
Conley et al. (2022) evaluated the dose-response curves for range of effects in rat dams and their offspring from dosing with PFOA and PFOS alone and in combination during gestation and early lactation. Mixtures of PFOA and PFOS caused effects at lower doses compared to PFOA alone for endpoints including decreased offspring survival; maternal and offspring body weight; offspring serum T3 and glucose; and increased maternal kidney weight; maternal and offspring liver weight; and offspring bile acids, BUN, and bilirubin. Histopathological changes were observed in maternal liver and kidney and offspring liver after exposure to the mixture. The effect of co-exposure to PFOA and PFOS for effects in dams and offspring was consistent with dose additivity, with the exception of maternal body weight at term and gestational weight gain, which were less than additive. USEPA (2023) stated that “this work is ongoing with multiple KE analyses still to be conducted on samples collected during the studies. However, results thus far support the hypothesis of joint toxicity on shared endpoints from PFOA and PFOS co-exposure, and dose additivity as a reasonable assumption for predicting mixture effects of co-occurring PFAS.”
Complex Mixtures—AFFF
McDonough et al. (2020) evaluated several endpoints in mice associated with exposures to a commercial AFFF formulation containing known concentrations of PFOS and PFOA. The results were compared to those from an unexposed control and another set exposed to a similar concentration of PFOA alone. The study identified elevated concentrations of several other perfluorosulfonic acids in the exposed mice compared to the controls, and statistically significant increases in liver mass. T-cell dependent antibody suppression in mice exposed to an AFFF dose, expressed as PFOS + PFOA, was comparable to that of an equivalent dose of PFOA alone, both of which were statistically significant in comparison to the control group. Blood serum analysis of the mice exposed to the AFFF showed that they had also been exposed to a range of perfluorosulfonic acids from PFPeS to PFDS, though PFHxs and PFOS were predominant.
Receptor Activation
As discussed in Section 17.2.5, an important MOA for many PFAS is activation of cellular receptors, including PPAR-α and others, that regulate expression of genes that control many biological pathways. Wolf et al. (2014) studied PPAR-α activation by PFOA, PFNA, PFHxA, PFOS, and PFHxS singly, and in binary mixtures of PFOA with each of the other four PFAAs using a cultured cell line transfected with the PPAR-α receptor. They concluded that there was additivity for PPAR-α activation in PFAS mixtures at concentrations up to 32 µM. An earlier study from the same research group used this test system with higher concentrations of PFAAs and found that PPAR-α activation in binary mixtures of PFOA, PFOS, PFNA, and PFHxS was antagonistic in the mixture of all four PFAS (Carr et al. 2013).
Activation of the estrogen and androgen receptors by PFOA, PFNA, PFDA, PFUnA, PFDoA, PFHxS, PFOS individually, and an equimolar mixture of all seven PFAAs, was evaluated in cultured cell lines transfected with these receptors (Kjeldsen and Bonefeld-Jorgensen 2013). The results of this study illustrated the complexity of interactions of mixtures of PFAS in regard to receptor activation. PFOA, PFOS, and PFHxS singly, as well as the mixture of the seven PFAAs, were weak agonists of the estrogen receptor and also enhanced activation by the endogenous estrogen, 17-beta estradiol. These three PFAS also inhibited activity of the androgen receptor, and the same three PFAS, as well as PFNA and PFDA, antagonized activation by the endogenous androgen, dihydrotestosterone. In contrast to some of the individual PFAAs, the PFAA mixture did not affect androgen receptor activity in the absence of dihydrotestosterone, but it did antagonize activation of the receptor by dihydrotestosterone. Comparison of the androgen receptor dose-response data for the inhibitory PFAAs and the mixture indicated a synergistic antagonistic effect (greater than additive inhibition) of the PFAAs in the mixture.
Nielsen et al. (2022) developed an in vitro system to predict the effects of defined PFAS mixtures on activation of human PPARα. They determined that PFCAs tended to act as full PPARα agonists and PFSAs tended to act as partial PPARα agonists, with individual PFAS differing in potency. Nielsen et al. (2022) also found that concentration additive approaches to predicting mixtures effects on PPARα may overpredict the effects of PFAS mixtures on PPARα activation.
Effects in Cultured Hepatocytes
Defined PFAS mixtures
The effects of PFHpA, PFOA, PFNA, PFDA, PFHxS, and PFOS individually, and in 11 binary and 4 ternary mixtures on cell viability of the human liver cell line, HepG2, were evaluated by Ojo et al. (2020). The concentrations that were tested for each PFAS were based on dilutions of the concentration that caused 50% loss of cell viability. Effects of many binary and ternary combinations were synergistic, while other combinations were antagonistic at some concentrations. PFOS was synergistic with the other five PFAS at almost all concentrations, while interactions in mixtures that included PFOA were either synergistic or antagonistic, with synergism predominating at lower concentration levels. In another study of the same cell line, PFOA and PFOS induced and promoted apoptosis, and a mixture of both PFAS showed additivity for this effect (Hu and Hu 2009).
Effects on gene expression of six individual PFAS (PFOA, PFNA, PFDA, PFDoA, PFOS, 8:2 FTOH) and four mixtures (PFOA plus PFOS; three mixtures of all six PFAS in different proportions) were evaluated in primary cultures of hepatocytes from rare minnow (Wei et al. 2009). No clear patterns of response were observed, in those mixtures of PFAS affected the expression of some genes that were not affected by individual PFAS, and vice versa.
Complex Mixtures—AFFF
Ojo et al. (2022) evaluated the toxicity of 24-hour exposure to varying concentrations of two historically used AFFFs containing PFAS in the HepG2 human liver cell line. PFAS in one of the AFFFs were primarily long- and short-chain PFAAs, while PFAS in the second AFFF were at lower concentrations and was primarily 6:2 FTS. Both AFFFs caused concentration-dependent decreases in cell viability and increases in two biochemical markers of toxicity; the AFFF containing PFAAs was more potent for these effects. Cellular DNA damage was induced only at the highest concentration tested (0.038%) of the AFFF containing PFAAs.
Zebrafish Studies
Defined PFAS mixtures
Fey et al. (2022) evaluated the effects of varying concentrations of PFOS and 6:2 FTS singly and as a mixture on mortality, hatching, and developmental endpoints in zebrafish. The authors concluded that the relative potencies of PFOS and 6:2 FTS in this study were not constant and varied at different concentrations of the test substances, and, therefore, dose additivity could not be assumed.
The lethality of PFOA, PFOS, and a mixture of both chemicals was studied in zebrafish embryos (Ding at al. 2013). The interaction between PFOA and PFOS was concentration-dependent, with additive, synergistic, antagonistic, and then synergistic effects observed as the proportion of PFOS was increased.
Behavioral effects in zebrafish embryos were evaluated for PFPeA, PFHxA, PFHpA, PFOA, PFNA, PFBS, PFHxS, PFOS, and 6:2 FTSA individually, and with mixtures of equal concentrations of all nine PFAS (Menger et al. 2020). PFHpA, PFOA, PFNA, PFHxS, PFOS, and 6:2 FTSA alone, as well as the mixture, caused behavioral effects in tests of locomotor activity, while PFBA, PFHxA, and PFBS did not. Specific behavioral effects varied among individual PFAS. The mixture of PFAS was less potent than the individual PFAS present in the mixture, suggesting antagonistic interactions among the PFAS in the mixture.
17.2.7.3 Studies of Mixtures of PFAS and Contaminants Other than PFAS
Several additional studies evaluated toxicological interactions of individual PFAS with other environmental contaminants. In male mice, co-exposure to PFOS and PCB126 (a dioxin-like PCB) caused synergistic effects on hepatic expression of genes related to oxidative stress, inflammation, and atherogenesis; levels of a protein that is a biomarker for thrombosis and fibrosis (indicators of cardiovascular disease risk); and hepatic lipid levels. Co-exposure, but not the individual compounds, caused pathological changes indicative of liver injury.
The effects on gene expression in zebrafish embryos of PCB126 alone, PCB126 plus PFOS, PCB126 plus PFHxA, and PCB126 plus both PFOS and PFHxA were evaluated by Blanc et al. (2017). The PFAS were not tested in the absence of PCB126. PCB126 with both PFOS and PFHxA had a greater effect on the expression of several genes than PCB126 alone or PCB126 with PFOS or PFHxA individually. The results suggest synergistic effects of PFOS and PFHxA on the effects of PCB126 in this test system.
17.2.8 Evaluating PFAS Using New Approach Methodologies
In one of its most resource-intensive efforts on PFAS to date, the USEPA developed a screening library containing PFAS. This USEPA-curated list spanned several public-interest lists of PFAS, including those from the USEPA, United States Food and Drug Administration (FDA), Department of Defense (DOD), Agency for Toxic Substances and Disease Registry (ATSDR), Consumer Product Safety Commission (CPSC), and state regulatory agencies. The screening library was developed to support the development of analytical methods, environmental monitoring, and toxicity testing. Further information on the initial list of 430 PFAS is available on USEPA’s CompTox Chemicals Dashboard (USEPA 2020), which was developed by the USEPA’s Chemical Safety for Sustainability Research Program (USEPA 2020). The purpose of the dashboard, along with related databases and web applications developed by the agency, is to support the USEPA’s computational toxicology research efforts to develop new and innovative methods with the goal of incorporating advances in a wide variety of scientific disciplines (biology, biotechnology, chemistry, and computer science) to help identify important biological processes that may be disrupted by chemicals. Using computational toxicology research methods, it is hoped that thousands of chemicals can be rapidly evaluated for potential risk at small cost, and chemicals can be prioritized for further studies based on potential health risk information derived from this initial evaluation (USEPA 2020).
From the initial list of 430 PFAS (discussed above), a subset of 150 PFAS were chosen by USEPA with the overall goals of maximizing the ability to perform read-across (for example, predicting toxicity of a target PFAS compound by extrapolating such information from a PFAS compound that has been more extensively studied) and capturing structural diversity among PFAS. The USEPA also took into consideration likelihood of exposure or occurrence, and the availability of in vivo (mammalian) or in vitro (for example, cell culture) toxicity data for validation. Because compounds that exist as gases cannot be tested and some PFAS (for example, HFPO-DA [GenX]) rapidly degrade in dimethyl sulfoxide (DMSO), which is used as the vehicle in many of these assays (Liberatore et al. 2020), practical considerations such as the ability to procure in nongaseous form and to solubilize samples in the solvent DMSO without degradation were also considered (Patlewicz et al. 2019; USEPA 2020, 2020).
This group of 150 PFAS is also currently being evaluated at Oregon State University, the University of Pittsburgh, East Carolina University, and other institutions in a USEPA-funded effort to use in vivo and in vitro methods to systematically study PFAS toxicity. The goal of this research is to support the prioritization of PFAS in risk assessment and risk management (USEPA 2019) by using a combination of in vivo toxicity screening assays and transcriptomics (evaluation of changes in RNA expression in specific tissues in response to biologic or environmental cues; these RNA molecules often code for proteins) in the zebrafish model to characterize the toxicity and pharmacokinetics of a range of volatile and nonvolatile PFAS. The subset of 150 PFAS is also being evaluated in in vitro assays intended to be predictive of various endpoints such as hepatotoxicity, developmental toxicity, immunotoxicity, neurotoxicity, mitochondrial toxicity, developmental neurotoxicity, endocrine disruption, and general toxicity (USEPA 2019). Results of these studies will be used to group PFAS by structures and biological activity. As mentioned above, the intent is to capture the structural diversity across the spectrum of PFAS of interest to USEPA and to support determination of the feasibility of read-across within structure-based groupings, an approach in which information from PFAS with extensive in vivo toxicity data could be used to predict toxicity of other PFAS that lack such data.
It is hoped that the results of these high throughput assays will (a) inform PFAS hazard characterization, (b) provide toxicokinetic information that may help predict disposition and excretion of PFAS from the body, and (c) prioritize PFAS for risk assessment and further in vivo mammalian testing that is needed for risk assessment. A further goal of this program is to determine, based on data for PFAS that have been evaluated in both in vitro and mammalian in vivo systems, whether the read-across approach can be used to support in vitro to in vivo extrapolation for estimation of oral equivalent exposures for PFAS (Fenton et al. 2020).
17.2.9 Data Gaps and Research Needs
Although many studies relevant to health effects of PFAAs have become available in the last few years, important data gaps remain for most of the PFAAs and PFECAs discussed here, as well as for many additional PFAS used in commerce or found in AFFF.
Human half-lives and other toxicokinetic data are not available for some PFAS found in drinking water and other environmental media. This information is critical for adequately assessing the bioaccumulative potential and relevant routes of exposure (for example, placental and breast milk transfer), and for extrapolation of animal toxicity information to humans.
Available data suggest that reactive intermediates can form in the metabolic pathways that convert PFAA precursors to PFAAs within the body. Additional information on the formation and potential toxicity of these reactive intermediates is needed.
Additional toxicology data are needed for some PFAAs found in environmental media, including drinking water. For example, there are very limited toxicology data for PFHpA, and no information was located for PFPeA. Additionally, although humans are exposed to multiple PFAS, very little toxicological data are available for mixtures of PFAS. Multigeneration studies are important for assessment of reproductive and developmental effects, and they are available for only a few PFAS. PFHxS is a PFAA with a long human half-life that has been found in human serum and in drinking water impacted by both industrial discharges and AFFF. Although developmental effects of PFHxS are of concern, there are currently no multigenerational developmental studies for PFHxS. Available information from rodent studies suggests that developmental exposures to some long-chain PFAS (PFOA, PFOS, PFHxS) cause permanent neurobehavioral effects, but these data are limited. Additional studies are needed on neurobehavioral effects of PFAS, particularly from early life exposure.
Studies that provide data on chronic effects, including carcinogenicity, are available for only four PFAS (PFHxA, PFOA, PFOS, GenX), and such studies are needed for PFHxS, PFNA, ADONA, and other PFAS to which humans may be exposed. All of the chronic studies were conducted in rats, and chronic studies in a second species such as mice would provide valuable information, particularly for those PFAS that are rapidly excreted in female rats.
The mode(s) of action for the toxicological effects of PFAAs are not fully understood and continue to be the focus of ongoing research. Although not the focus of this section, data on bioavailability of PFAS from environmental media other than drinking water (for example, soil) are limited, and such information can be useful in assessing exposures at contaminated sites.
Challenges related to the use of toxicity information from surrogates for PFAS for which no toxicity data are available are discussed in Section 9.1.1.2. There is a need to further develop and validate approaches for addressing groups and mixtures of PFAS, such as those described in Section 17.2.7.
Finally, OECD (2018) identified 4,730 PFAS-related CAS numbers, including compounds with many different structures, including some that have not been used commercially. The majority of these PFAS, including those in commercial use, have very limited or no toxicity data (Wang et al. 2015; Wang et al. 2017), indicating a critical data gap in health effects information for PFAS. The approaches currently under development at USEPA and the National Toxicology Program (NTP) that are discussed in Section 17.2.8 may prove useful for screening of a large number of PFAS with rapid assays that evaluate parameters related to toxicokinetics and toxicity (USEPA 2018). Additional information is found on the USEPA CompTox website (USEPA 2020; Williams et al. 2018) and from the NTP Rapid Evaluation and Assessment of Chemical Toxicity (REACT) Program (DeVito 2018). If this effort is successful, the results could be used, along with data on human exposure, for prioritization of PFAS for more detailed toxicological studies (USEPA 2018).
17.3 Additional Information for Risk Assessment
17.3.1 Human Health Exposure Assessment
Figure 9-5 illustrates predominant exposure pathways. In the following sections, summary information is presented for exposures by environmental medium. Information about site risk assessment is in Section 9. Information about PFAS occurrence in environmental media is discussed in Section 6. Links are provided to other sections for more details on related topics.
17.3.1.1 Soil
Soil exposure scenarios are possible at a site. Many PFAS are mobile and persistent in soil. As indicated in Section 5, PFAS distribution in soils is complex, reflecting several site-specific factors and individual PFAS-specific factors.
Sorption and retardation generally increase with increasing perfluoroalkyl tail length, and functional groups contribute to the degree to which a PFAS has the affinity to leach from soil to groundwater. A detailed discussion of the fate of PFAS in soil is provided in Section 5. Receptors, such as humans, terrestrial animals, and plants, in contact with soil containing PFAS may be exposed to the compounds.
PFAS may be absorbed through the skin; some relevant studies are summarized in Section 17.2.3, Section 1.4.3, and by ATSDR (2021). Therefore, current evidence combined with existing toxicity factors suggest that dermal absorption from soils or associated groundwater is not expected to be an important exposure route for the general public compared to other exposure pathways, but may contribute to less significant exposures such as incidental ingestion of soils in combination with skin contact. Construction workers may contact PFAS in soils (if within the depth of construction activities).
17.3.1.2 Potable Water
Ingestion of PFAS-containing drinking water typically represents the dominant exposure pathway in comparison to ingestion of food or other exposure pathways especially when PFAS concentrations in drinking water reach a certain level (Post, Gleason, and Cooper 2017; Bartell 2017). Section 1.4.1 includes information about potential human health effects from PFAS exposure arising from AFFF in drinking water. However, the dominance of the drinking water pathway is relative and can be context specific as highly contaminated sources of food (e.g., fish or agricultural products) might result in significant exposure greater than that of water. As discussed and cited in Section 7.1.2, PFAS levels in young children (up to the age of 6) are often higher than in adolescents and adults consuming the same drinking water source (see also Section 17.2). This is most likely due to the relatively higher levels of water ingestion per unit of body mass at these ages. If bottled water is supplied for drinking water and food preparation purposes, potential exposures from potable water used for non-drinking water purposes (for example, showering, bathing, and hand-washing dishes) are expected to be minimal, with the possible exception of inhalation exposure to volatile PFAAs (see Section 17.3.1.6), which is not yet well characterized.
17.3.1.3 Groundwater
The same potential exposure pathways described above for potable water apply to groundwater when used as a potable source. As discussed for soils, construction workers may contact PFAS in shallow groundwater (if within the depth of construction activities), although dermal absorption potential from water is low. If PFAS-impacted groundwater is used as irrigation water for crops, homegrown produce, or animal watering, PFAS in groundwater may be transferred to biota (plants or animals), resulting in potential dietary exposures (see Section 17.3.3).
As indicated in Section 5.3, due to the mobility and persistence of PFAS in soil and groundwater, certain PFAS are expected to form larger plumes than certain less-soluble contaminants in the same hydrogeological setting. However, sorption and partitioning might restrict leaching rates from the vadose zone and reduce the advection-driven transport velocity of PFAS in groundwater, depending on specific properties of the PFAS. These processes might limit plume development and discharge to surface water and might provide time for transformation of PFAS precursors. Groundwater geochemistry can also affect the extent of biotic and abiotic transformation of PFAS precursors (Liu and Mejia Avendaño 2013).
17.3.1.4 Surface Water
Surface water impacted with PFAS by surface runoff or groundwater discharge also present possible exposures. Surface water exposures can occur through drinking water or by consuming aquatic biota from contaminated water bodies. Much of the PFAS reaching surface water tend to remain in solution, although there is likely to be partitioning to sediment and uptake to biota. Once in surface water, PFAS could contaminate groundwater through groundwater recharge (Liu et al. 2016; ATSDR 2008). See Section 16.2 for human health aspects of PFAS in surface water. The Priority Topics for Fate and Transport, Surface Water, Source ID, and Site Characterization include information about PFAS in marine environments (see Section 1.3.5) and the effects of suspended sediment on surface water sampling and measurement of PFAS (see Section 1.3.6).
Biofilms on surface water are known to accumulate PFAS (Munoz et al. 2018), as do other organic-/protein-rich particles in aquatic systems (Ahrens and Bundshuh 2014). Therefore, surface water films that contain these matrices could be repositories (and potential sources of exposure), especially of long-chain PFAS. Similarly, PFAS-containing foams may form on certain surface waters and contribute to recreational exposures. PFAS-containing foam is discussed in Section 16.5.
17.3.1.5 Sediment
PFAS in surface runoff or groundwater discharge can partition to sediment and be taken up into biota. The exact processes that control affect sorption and bioavailability of PFAS in sediments are poorly understood and likely determined by several factors including the mixture of PFAS, salinity, and sediment composition (see Sections 6.5 and 5.3.4.2). Considerations for PFAS in sediments and the potential implications for human health risk assessment (for example, bioaccumulation into fish and recreational contact) are detailed in Sections 9.1 and 16.2.
17.3.1.6 Air
PFAS inhalation exposure scenarios are possible. Examples include dusts containing PFAS may be generated from a site where PFAS are present in soil, as well as aerosols derived from surface waters (Section 5.2.4). In addition, some PFAS (for example, FTOHs and some perfluoroalkyl sulfonamides) have higher volatilities and can partition into air from other media (Section 5.2.4). Certain PFAS are found in ambient air with elevated concentrations observed or expected in urban areas near emission sources, such as manufacturing facilities, wastewater treatment plants, fire training facilities, and landfills (Barton et al. 2006; Ahrens et al. 2011; Liu et al. 2015). See Section 6.1 for more information about PFAS occurrence in air. See also the PFAS and Vapor Intrusion Fact Sheet developed in 2025.
17.3.1.7 Diet
PFAS exposures may occur from food consumption, such as ingesting aquatic and terrestrial plants and animals that have taken up PFAS. Crops may be impacted by PFAS if irrigated with contaminated groundwater or surface water; if impacted by soil, runoff, or atmospheric deposition; or where biosolids have been applied to soil. In addition, because some PFAS biomagnify in food webs, ingestion of contaminated biota, especially fish and animals that eat fish, may be an important exposure route (ATSDR 2020; ATSDR 2021; USEPA 2016; USEPA 2016). Recreationally caught fish from areas with PFAS contamination may be a specific source of elevated exposures to PFAS that bioaccumulate in fish. PFAS exposures may also occur from food packaging materials containing PFAS (see Section 17.3.1.8, Consumer Products). The Priority Topics for Biosolids Land Application (see Section 1.7) include information about potential risks from agricultural impacts, plant uptake, and uptake by animals.
Breast Milk and Infant Formula
Consumption of breast milk and infant formula are potential exposure scenarios for infants. Breast milk may be impacted from a lactating mother’s exposure to PFAS-contaminated media, and infants may ingest PFAS from formula prepared with PFAS-contaminated water (Fromme et al. 2010; Mogensen et al. 2015). Higher exposures to infants are of concern because infants are sensitive subpopulations for developmental effects of PFAS, as discussed in Section 7.1 and Section 17.2. Infants may have a higher level of exposure to PFAS through breast milk or formula prepared with contaminated water than adults typically have through consuming contaminated water due to differences in the volume of water consumed relative to body weight. The USEPA Exposure Factors Handbook (USEPA 2019) provides detailed information on breast milk consumption rates and the higher water consumption rate of infants.
17.3.1.8 Consumer Products
Typically, exposure scenarios associated with consumer products are not included in human health risk assessments (HHRAs) for contaminated sites. However, the HHRA should acknowledge that analytical results for environmental media (including indoor air and dust) may reflect impacts from consumer products (for example, carpets and upholstered furnishings) containing PFAS that have degraded, released fibers, or volatilized (see Section 2.5). Section 1.4.2 includes information about potential PFAS exposures from consumer products.
17.3.2 Other Considerations When Calculating Exposure Point Concentrations
Other contaminants present at the site can affect the movement of PFAS, which are not easily accounted for in fate and transport models. For example, petroleum hydrocarbon co-contaminants, particularly light nonaqueous phase liquids (LNAPLs), may affect the fate and transport of AFFF-derived PFAS (Guelfo and Higgins 2013; Lipson, Raine, and Webb 2013; McKenzie et al. 2016). As discussed in detail in Section 5 and Section 10.4, PFAS movement in environmental media depends on both site-specific media properties and properties of the specific PFAS. Leaching potential is a function of both media properties (for example, pH, redox conditions) and PFAS structural properties (for example, chain length) (Gellrich, Brunn, and Stahl 2013; Gellrich, Stahl, and Knepper 2012).
It is critically important to collect site-specific soil partitioning and soil-to-groundwater pathway data for PFAS sites. Existing models and standard methods are not able to accurately predict or calculate soil-to-groundwater movement of PFAS given their hydrophobic and hydrophilic properties. Therefore, site-specific empirical data are necessary.
As discussed in detail in Section 5.4, the composition of PFAS can change in media. Studies have reported both biotic and abiotic transformations of some polyfluorinated substances (precursors), which may form PFAAs (Buck et al. 2011). Precursors that are ingested can be transformed in the body to PFAAs (USEPA 2016; USEPA 2016). However, PFAAs likely do not degrade or otherwise transform under ambient environmental conditions. PFAS composition may also change in surface water because of biotic and abiotic degradation of PFAA precursors. These complex transformations are not incorporated in current fate and transport models.
17.3.3 Information about Selecting Bioaccumulation and Bioconcentration Factors
Certain PFAS can bioaccumulate in the food web including aquatic organisms (see Section 5.5 [PFAS Uptake into Aquatic Organisms] and Section 6.5.3 [Fish]), terrestrial animals (for example, livestock and wild game), as well as plants. PFAAs, particularly PFOS, are typically the dominant PFAS detected in biota (Houde et al. 2011). Section 5.5, 5.6, and Section 16 provide detailed discussions of factors affecting the bioaccumulation potential of PFAS across a variety of organisms. The Priority Topics for Biosolids Land Application include information about plant uptake (see Section 1.7.4) and uptake by animals (see Section 1.7.5).
Figure 17-1 illustrates bioaccumulation pathways from sediment and surface water.
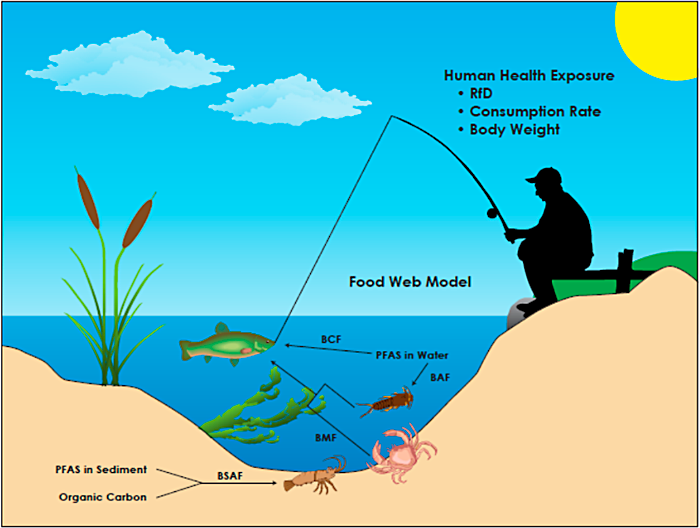
Figure 17-1. Bioaccumulation of PFAS from sediment and surface water. (BAF–bioaccumulation factor; BCF–bioconcentration factor; BSAF–biota-sediment accumulation factor; BMF–biomagnification factor; RfD–reference dose.
(Source: J. Conder, Geosyntec. Used with permission.)
Section 6.5.3 (Fish) provides a detailed discussion of bioaccumulation of PFAS in fish. PFAS accumulation in fish has been documented, particularly for PFOS, longer chain PFCAs (with eight or more fluorinated carbons), and perfluorodecane sulfonate (PFDS) (Houde et al. 2011; Martin et al. 2013; Conder et al. 2008). In fish, PFOS tends to partition to the tissue of highest protein density, including the liver, blood serum, and kidney (Falk et al. 2015; Ng and Hungerbühler 2013). Available aquatic organism BCF and BAF data are presented in Table 5-1 (provided as a separate Excel file). Trophic level biomagnification in food webs (Figure 17-1) can occur for some PFAS (Franklin 2016; Fang et al. 2014) as discussed in further detail in Section 5.5.3.
Sections 5.6 and 6.5.1 discuss partitioning of PFAS to plants. 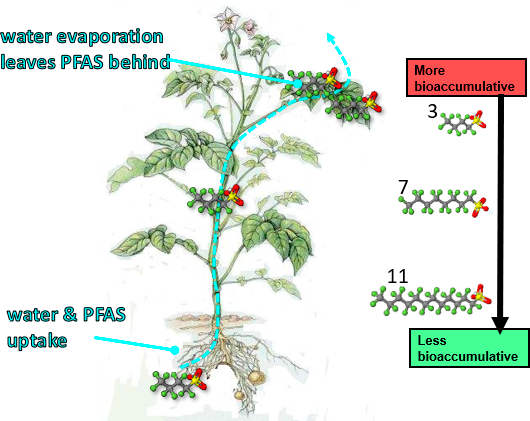
Figure 17-2. Bioaccumulation of PFAS in plants.
Source: J. Conder, Geosyntec. Used with permission.
Plant uptake, bioaccumulation, and partitioning within the plant appear to depend on PFAS chemical structure and the plant species. Figure 17-2 illustrates bioaccumulation of PFAS in plants. Most studies report partitioning of PFAAs within plants, with longer chain PFAAs, especially PFSAs, partitioning to the roots and more soluble, shorter chain PFAAs, especially PFCAs, partitioning to other parts of the plant (Lechner and Knapp 2011; Stahl et al. 2009) Blaine (Blaine et al. 2013; Blaine, Rich, Sedlacko, Hundal, et al. 2014; Yoo et al. 2011; Scher et al. 2018; Gobelius, Lewis, and Ahrens 2017). Table 5-2 (provided as a separate Excel file) contains BCFs and BAFs for various PFAS in a variety of plant species. In general, most plant BCFs and BAFs fall between a range of 0.1 and 10.
As indicated in Section 4.2.8 (Octanol/Water Partition Coefficient (Kow)) and Section 5.5.2 (Bioaccumulation), it is difficult to measure Kow for PFAS due to their complex chemistry, and because many PFAS have both hydrophilic and hydrophobic properties. Therefore, BAFs rely on calculations from empirical data instead of modeling (Haukås et al. 2007).
–
Updated January 2026.

